Main risk factors associated with surgical site infection in adult patients treated in a general surgery service
Andrea Padilla-Morán and Eduardo Arturo Serrano-García
Hospital General de Zona No. 14, Instituto Mexicano del Seguro Social, C. República de Cuba, El Mirasoles, 83120 Hermosillo, Sonora, México.
Abstract
Introduction: Surgical site infections (SSIs) account for 20% of all healthcare-associated infections (HAIs). After a surgical procedure, one-third of patients will contract one. Consequently, this results in a 7- to 11-day increase in hospital stay and a 2- to 11-fold increased risk of death compared to operated patients who did not contract one. This triggers a significant increase in morbidity, hospital stay, and costs.Objetive: To identify the main risk factors associated with the presentation of a surgical site infection (SSI) in adult patients undergoing surgery in the general surgery service.
Materials and methods: This is an observational, analytical, retrospective, and cross-sectional case-control study nested within a cohort. A review of medical records and databases will be conducted. A non-probability sample of consecutive cases will be used to determine if there is a correlation between them, using contingency tables to obtain odds ratios.
Results: The odds ratios (OR) with statistical significance for BMI were normal 0.365 (95% CI 0.130 - 1.027, p 0.050), overweight 0.273 (95% CI 0.126 - 0.592, p<0.001), and grade I obesity 4.571 (95% CI 2.032 - 10.284, p 0.001). A previous healthcare-associated infection (HAI) was found in 28.3% of cases and in 5% of controls, with an OR of 7.512 (95% CI 2.068 - 27.278, p 0.001).
Conclusions: Although there are situations both before and during the surgical procedure that can be difficult to control, this study demonstrates that those that are controllable and applicable by health personnel can become more relevant.
Keywords: Infections, surgical site, surgeries, risk factors.
INTRODUCTION
The World Health Organization (WHO) defines Healthcare-Associated Infections (HAIs) as infections that affect a patient during care in a hospital or healthcare facility, which were not present or incubating at the time of admission and which may even manifest after the patient's discharge.
They are considered one of the major global health problems, compromising patient safety and directly impacting the quality of care in healthcare facilities.
Surgical Site Infections (SSIs) account for 20% of all HAIs. It is estimated that after a surgical procedure, approximately one-third of patients will contract one. This can lead to an increase of 7 to 11 days in hospital stay and a 2 to 11-fold increased risk of death compared to surgical patients who did not contract an infection. This results in a significant increase in morbidity, hospital stay, and costs.
Surgical site infections (SSIs) account for 20% of all healthcare-associated infections (HAIs) in a hospital unit. It is expected that after a surgical procedure, one-third of patients will develop an SSI, resulting in a 7- to 11-day increase in postoperative hospital stay and a 2- to 11-fold increased risk of death compared to surgical patients who did not develop an SSI.1
While the causes of SSI development are multifactorial, they are a strong indicator of the quality, safety, and efficiency of healthcare services. Timely identification of predisposing risk factors and appropriate application of preventive measures leads to a decrease in morbidity and mortality, and consequently, in the costs associated with prolonged hospital stays, additional surgical procedures, and antimicrobial use.2
The Ministry of Health, through the Hospital Network for Epidemiological Surveillance (RHOVE), has published definitions of healthcare-associated infections (HAIs) in the "Manual of Standardized Procedures for Hospital Epidemiological Surveillance, RHOVE," with the aim of standardizing clinical and laboratory criteria, and thus ensuring proper surveillance, prevention, and control of these infections.5 The Mexican Social Security Institute (IMSS) also maintains the Healthcare-Associated Infection Registry System (INOSO), where HAIs detected through active and passive surveillance by Hospital Epidemiological Surveillance Units (UVEH) are recorded.
In both platforms, consistent with global statistics, surgical site infections (SSIs) constitute 20 to 30% of all healthcare-associated infections (HAIs) reported annually. They were among the top ten reported infections, out of the twenty-five defined, during 2022, and the leading cause of infection in the General Surgery department.6
Surgical site infections (SSIs) are defined as infections that occur at the site of an incision, which may involve skin, subcutaneous tissue, fascia, muscle, organs, spaces, or implants. They can occur within the first 30 days or up to a year after surgery, depending on the type of infection and the surgery performed.7 SSIs are classified as follows: superficial incision, deep incision, and organ/space incision.7
Not all surgeries will have the same degree of contamination at the time of the procedure; therefore, it is useful to categorize them to facilitate comparisons and adjust SSI rates.7 These classifications are clean, clean with implant, clean-contaminated, contaminated, and dirty or infected. 7
Several pathophysiological factors are known to contribute to surgical site infections (SSIs), which can be divided into factors related to the surgical procedure, microbial factors, factors related to adherence to preventive practices, and patient-related factors.8
In Mexico, the Hospital Epidemiological Surveillance Network issued an Epidemiological Overview in August 2022 regarding healthcare-associated infections (HAIs) reported in the country. From January 1 to August 31, 2022, a total of 36,425 HAIs were reported. For the General Surgery service alone, 5,959 SSIs were registered across all classifications.6
The Ministry of Health and the Mexican Social Security Institute (IMSS) consider SSIs to be among the priority pathologies to be identified promptly, in order to act as quickly as possible and thus reduce the risks identified in critical procedures. Establishing continuous improvement processes that contribute to the prevention of risks, adverse events, and sentinel events arising from healthcare processes.
The objective of this study was to identify the main risk factors associated with the development of surgical site infections in adult patients undergoing surgery in the general surgery department.
MATERIALS AND METHODS
The study took place at General Hospital No. 14, located in Hermosillo, Sonora. It is a Level II Care Unit with 326 available beds; of which 200 are authorized (census beds) and 126 are unauthorized (non-census beds). It also has 36 consulting rooms, 1 emergency room, 3 information modules, 5 inpatient services, 8 operating rooms, 1 administrative area, and a physical medicine and rehabilitation service.
A case-control study was conducted, where the cases were patients who underwent surgery and developed a surgical site infection (SSI) during the study period, and the controls were the same number of patients who underwent surgery during the same period but did not develop an SSI. Patients over 18 years of age, of both sexes, who underwent surgery between January 1 and December 31, 2022, were included. Patients under 18 years of age, patients who underwent surgery in a year other than 2022, patients treated in the gynecology and obstetrics service, patients treated in the orthopedics and traumatology service, patients who underwent surgery in another unit, and patients with surgical site infections not recorded on the INOSO platform were excluded. Patients with incomplete information in their electronic medical records, study population, and sample size were also excluded.
The independent variables included in the study were: age, pre- and postoperative hospital stay, systemic hypertension, type 2 diabetes mellitus, obesity, chronic kidney disease, cancer, rheumatoid arthritis, chronic infections, other comorbidities, surgical time, operating room, surgical specialty, surgical shift, preoperative diagnostic classification by organ systems, smoking, safe intervention packages for surgical site infection (SSI) prevention (defined as a series of interventions to be performed before, during, and after surgery, antibiotic prophylaxis, open or closed surgical approach, degree of surgical wound contamination, use of invasive methods (central venous catheter, mechanical ventilation, Foley catheter), and having a previous healthcare-associated infection (HAI) within the last 30 days.The dependent variable was surgical site infection, according to current regulations.
Data collection was retrospective and cross-sectional to obtain an overview of the unit's health status at a specific point in time. Data analysis was performed using SPSS v.24 statistical software. Quantitative variables for demographic characteristics were obtained using descriptive statistics such as means, modes, and proportions. Contingency tables were used to determine the correlation between independent and dependent variables, obtaining odds ratios with a 95% confidence interval. The chi-square test was then applied to verify statistical significance.
Based on the regulations of the General Health Law regarding health research, this research is without risk, as only patient data were collected and no invasive protocols that could harm the study subjects were performed. This study was conducted respecting the ethical codes established in the Declaration of Helsinki 1964, in its 2013 version, as well as those established in the Mexican Standards of the Official Gazette of the SSA of 1962.
RESULTS
One hundred surgical site infections were recorded during the study period. Based on the formula for two proportions, it was determined that the study population should consist of 25 cases. However, it was decided to use 100% of the cases registered on the INOSO platform. After applying the inclusion, exclusion, and elimination criteria, a total of 60 records were selected for the cases and 60 records for the controls.
The sociodemographic characteristics were as follows: 55% were women (n=33), and 45% were men (n=27). Regarding age, the mean age was 54.2 years. The patients' ages were classified into ranges, with the highest frequency in the 60-69 age range (21.7%) (Table 1).
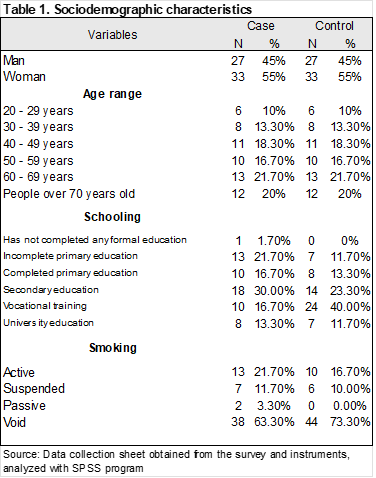
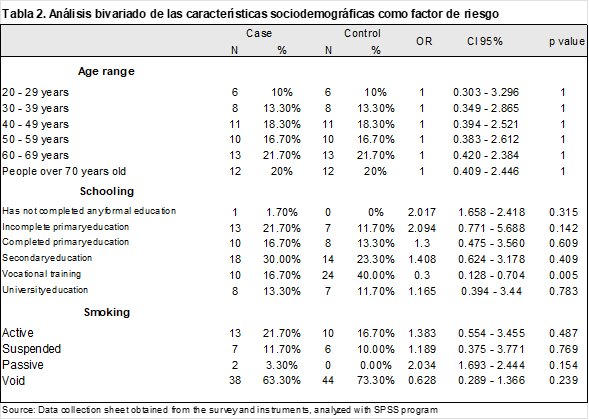
In the cases, the predominant educational level was secondary education (30%), while in the controls, it was middle school education (40%). An odds ratio (OR) was calculated for each educational level, finding that secondary education was a protective factor (OR 0.3, 95% CI 0.128–0.704, p-value 0.005) (Table 2).
The OR for active smoking was 1.383 (95% CI 0.732–3.461), with a p-value of 0.487, indicating no statistical significance (Table 2).
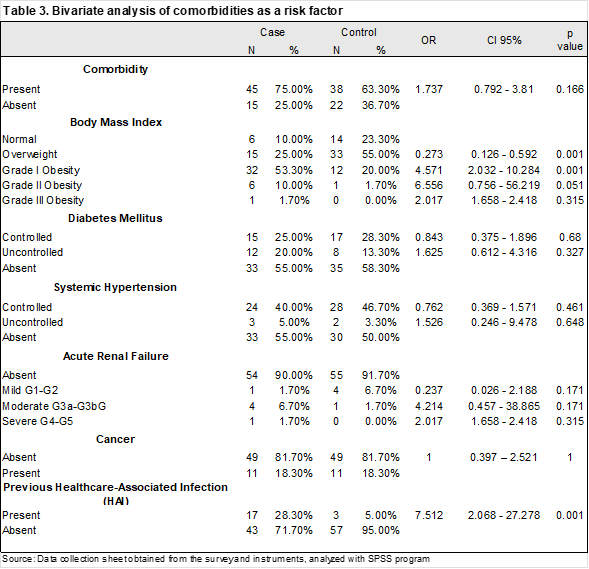
Analyzing comorbidities, the presence of comorbidity resulted in an OR of 1.737 (95% CI 0.792–3.81, p-value 0.166), also without statistical significance. Regarding BMI, grade I obesity predominated in the cases (53.3%), while overweight was the most common finding in the controls (55%). The statistically significant odds ratios (ORs) for BMI were normal 0.365 (95% CI 0.130–1.027, p < 0.050), overweight 0.273 (95% CI 0.126–0.592, p < 0.001), and grade I obesity 4.571 (95% CI 2.032–10.284, p < 0.001) (Table 3).
In addition, Diabetes Mellitus (DM) (OR 0.843, 95% CI 0.375–1.896, p = 0.680), Systemic Arterial Hypertension (SAH) (OR 0.762, 95% CI 0.369–1.571, p = 0.461), and chronic kidney disease (CKD) (OR 0.237, 95% CI 0.026–2.188, p = 0.171) were considered, which is not statistically significant. The frequency of cancer was 18.3% in both cases and controls (OR 1.000, 95% CI 0.397–2.521, p = 1.000). A prior healthcare-associated infection (HAI) was found in 28.3% of cases and 5% of controls, with an odds ratio (OR) of 7.512 (95% CI 2.068–27.278, p < 0.001), which was statistically significant. (Table 3)
Regarding the surgical event, in both cases and controls, the type of intervention was 56.7% scheduled and 43.3% urgent; the surgical approach was 90% open and 10% closed; and the classification of the degree of surgical wound contamination was 35% clean, 48.3% clean-contaminated, and 16.7% contaminated. The most frequent specialty was general surgery (88.3%), and the digestive system was the most affected (65%). The most frequent shift for cases was the morning shift at 36.7% (OR 2.316, 95% CI 1.018–5.269, p 0.043), and for controls, the afternoon shift at 53.3% (OR 0.375, 95% CI 0.183–0.771, p 0.007). Operating room Q1, with a frequency of 25% in cases and 10% in controls, yielded an OR of 3.000 (95% CI 1.075–8.370, p 0.031), which was statistically significant (Table 4).
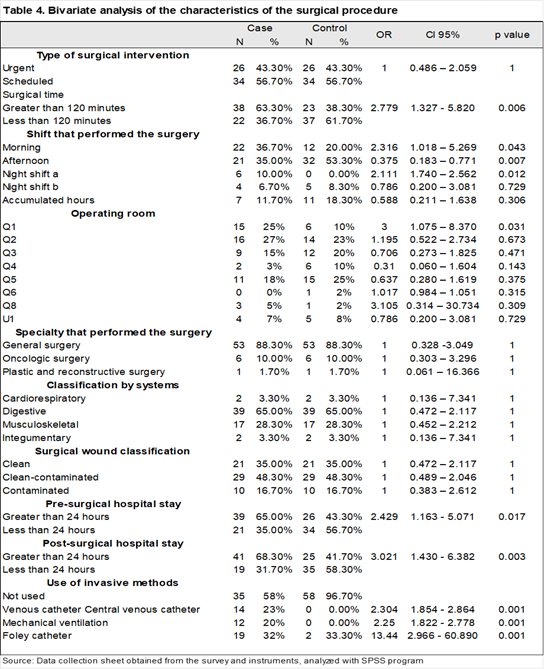
Surgical time exceeding 120 minutes yielded an OR of 2.779 (95% CI 1.327–5.820, p 0.006), which was also statistically significant. The pre-surgical stay yielded an OR of 2.429 (95% CI 1.163 - 5.071, p 0.017) and the post-surgical stay an OR of 3.021 (95% CI 1.430 - 6.382, p 0.003), both with statistical significance.(Table 4)
The use of invasive methods was found to have the following odds ratios: central venous catheter use (OR) 2.304 (95% CI 1.854–2.864, p < 0.001), mechanical ventilation (OR) 2.250 (95% CI 1.822–2.778, p < 0.001), and Foley catheter use (OR) 13.439 (95% CI 2.966–60.890, p < 0.001), all of which were statistically significant.(Table 4)
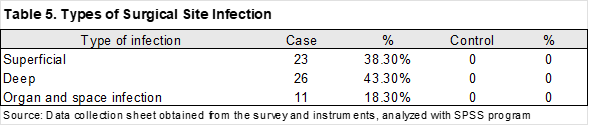
The frequencies of surgical site infections were classified as follows: 38.3% superficial, 43.3% deep, and 18.3% organ/space (Table 5).
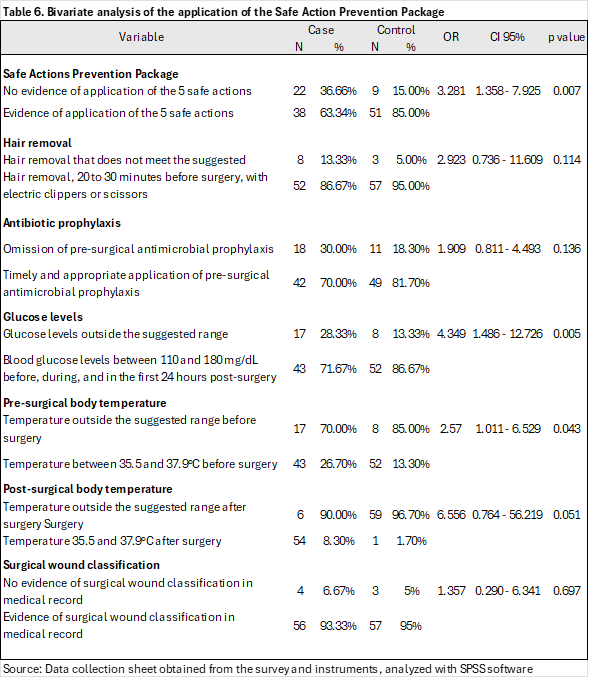
Omission of the prevention package represents an OR 3.281 (95% CI 1.358 - 7.925, p 0.007), with statistical significance. Failure to maintain glucose levels within the suggested ranges (OR 4.349, 95% CI 1.486 - 12.726, p 0.005) and failure to maintain preoperative temperature within the suggested ranges (OR 2.570, 95% CI 1.011 - 6.529, p 0.043) were also statistically significant.(Table 6).
DISCUSSION
According to the data obtained in this study, a 5% difference was found between sexes, with a frequency of 45% for males and 55% for females.
Analyzing the sociodemographic characteristics, for the age variable, the mean was 54.2 years and the median was 52.5 years, consistent with Peñuela in Colombia (201), who found a significant difference in patients over 54 years of age (OR 5.37; p 0.014)16. Fernández et al. in Cuba (2016) also corroborated that adulthood is a decisive non-modifiable factor in postoperative infections17.
For the education variable, having a high school diploma was found to be a protective factor against the development of a surgical site infection (SSI).
For BMI, grade I obesity was the most frequent category for cases, and overweight for controls. The odds ratio (OR) suggests obesity as a risk factor and overweight as a protective factor. This agrees with the findings of Hidalgo-Costilla et al. in Mexico in 2015, who established an OR of 2.234 (95% CI 1.563–3.194)18, and with those of Figuerola in Spain in 2016, who reported an association between surgical site infection (SSI) and obesity (OR 1.2; CI 1.0–1.4; p < 0.05).22
Although the results show that diabetes mellitus and systemic hypertension did not show statistical significance as a predisposition to developing a surgical site infection, there is evidence demonstrating this association, as in the case of García Díaz with 190 patients (OR 3.43; p 0.01)19. Another study by Ramos et al. indicates a significant association between diabetes and surgical site infection (OR 8.67; 95% CI 1.53-49.30; p 0.015).20
Chronic Kidney Disease, by itself, does not appear to represent a risk factor as such, but it could be associated with multiple complications that may precede a surgical site infection.3,5,8
Although in this study cancer was not investigated as a risk factor per se, but rather as a characteristic also present in the controls, Velasco et al. established this parameter as a predictive risk factor for SSI among patients with cancer (OR 3.76, 95% CI 1.76-8.03).21
A healthcare-associated infection in a previous area represents a significant risk for developing a surgical site infection, as the presence of a distant infection has been shown to increase the SSI rate by 2.7 times.24
Although the following characteristics were intentionally sought to be present in the same proportion in both cases and controls, there is evidence that there is a greater risk of developing a surgical site infection in urgent surgery than in elective surgery (Peru 2019, OR 1.26; CI 1.89-3.45; p 0.021)25, in an open approach than in a closed one (Colombia 2017, OR 3.62; CI 1.56-8.39; p 0.00, Spain 2018 RR 0.10; CI 0.01-0.79, p < 0.05, United States 2010 OR 0.28; CI 0.25-0.31)26,27,28, if the wound classification is clean-contaminated (Brazil 2017 OR 2.7; CI 2.1-3.5; p 0.001)29. Consequently, it is not difficult to believe that the service that presents the highest frequency of this condition is general surgery, as well as that the system with the highest frequency after an intervention resulting in an SSI is the digestive system, related to the fact that most of its procedures have these characteristics.
A surgical time exceeding 120 minutes was associated with a risk factor for surgical site infection (SSI), a finding confirmed in other studies. In 2017, Cheng et al., through a systematic review of several studies, found a statistically significant association, establishing that there is almost twice the likelihood of developing this type of infection.32
Regarding the surgical shift, the morning shift was the most frequent, establishing it as a risk factor, along with the night shift. On the other hand, for the control group, the afternoon shift was the most frequent, and it was found to be a protective factor. Operating room Q1 was identified as a risk factor for the development of an SSI.
Hospital stays exceeding 24 hours, both before and after surgical procedures, significantly increase the risk of surgical site infection (SSI). This finding was confirmed by Rodrigues (Brazil, 2017), who established a statistical relationship between a preoperative stay longer than 24 hours and SSI (OR 2.3; CI 2.0–2.8; p < 0.001).29
The use of invasive procedures has been shown to be a risk factor that can significantly increase the likelihood of developing a surgical site infection. This may be due to the invasive procedure itself creating an entry point for microorganisms, thus promoting infection, or to the susceptibility and comorbidities of patients requiring this type of management. However, there is no precedent confirming or ruling out the influence of invasive procedures on the development of SSIs, leaving an opportunity for further investigation.
Safe practice bundles for the prevention of surgical site infections (SSIs) comprise a series of tasks to be implemented by healthcare personnel. A substantial body of scientific evidence supports the significant reduction in the risk of developing SSIs.1,2,3,4,5,6,7,2 This study was no exception, as the characteristics attributed to healthcare showed statistical significance, including the analysis of the use of safe practice bundles.
Antibiotic prophylaxis did not demonstrate statistical significance; however, evidence from Gallagher et al. in a 2018 systematic review indicates that antibiotic prophylaxis likely reduces the incidence of SSIs (RR 0.67, CI 0.53–0.85).30 Despite this, other research studies disagree, such as that of Del Moral, who concludes that adequate antibiotic prophylaxis did not influence surgical site infection (RR 1.15; CI 0.31-2.99; p > 0.05)31.
Monitoring glucose levels between 110 and 180 mg/dL is the first safe step in the surgical site infection (SSI) prevention package. High stress levels, such as those experienced during surgery, combined with glucose levels below 110 mg/dL or above 180 mg/dL, cause abnormalities in monocyte and polymorphonuclear neutrophil function, decreased intracellular bactericidal activity, and glycosylation of immunoglobulins,33 which favor the development of infection. The results obtained are consistent with this, as in the HGZ 14 CUQ hospital, uncontrolled blood glucose was associated with a 4.3 times greater risk of developing an SSI.
Monitoring body temperature is part of the safe measures for preventing infections7,23, so it is expected that a temperature outside the suggested range (35.5 to 37.9°C) increases the risk of developing a surgical site infection (SSI) by 2.5 times.
While surgical wound classification is a parameter that helps determine the most appropriate therapeutic approach for the patient, as it can indicate the likelihood of complications, the lack of classification evidence in the medical record does not represent a statistically significant risk.
The microorganisms most frequently found in the cultures were primarily Escherichia coli, followed by Klebsiella pneumoniae, Pseudomonas aeruginosa, and Enterococcus faecalis. This coincides with the findings reported nationally by the DGE on the RHOVE6 platform. When studying the characteristics of patients with confirmed surgical site infections (SSIs), a majority had a secondary education or lower, and a significant number had a history of smoking.
Continuing with the analysis of past medical history, a significant portion of the sample presented comorbidities, such as obesity, diabetes mellitus, and systemic hypertension, and the poor control of these conditions was noteworthy.
Regarding the characteristics of the surgical procedure itself, elective surgeries were more frequent, as were open surgeries, with the majority of surgical wounds classified as clean-contaminated. However, the most relevant finding in this study was the application and adherence to safety protocols, which depend on the competence of the healthcare personnel. Therefore, there is an opportunity to implement these measures, which greatly contribute to the positive outcomes for patients. Although there are situations both before and during the surgical procedure that can be difficult to control, this study demonstrates that those controllable and applicable by healthcare personnel can be of greater importance. Therefore, it is crucial to continue training all medical staff on the importance of implementing these measures, showing them the impact on patient outcomes, the use of supplies, and hospital space, both when using them and when not.
REFERENCES
1.Prevention and diagnosis of surgical site infection. Evidence and Recommendations Guide: Clinical Practice Guideline. Mexico, Mexican Social Security Institute; 2018 [Accessed May 2023]. Available from: http://imss.gob.mx/profesionales-salud/gpc
2.Guanche Garcell H, Gutiérrez García F, Pisonero Socias JJ, Rubiera Jiménez R, Suárez Cabrera A. Prevention of surgical site infections in the training of medical students and general surgery residents. Cuban Journal of Higher Medical Education [Online]. [Published January 2023, accessed May 2023] Available from: https://libcon.rec.uabc.mx:5471/login.aspx?direct=true&db=lth&AN=142418621&lang=es&site=ehost-live
3.World Health Organization. Pan American Health Organization. Epidemiological Surveillance of Healthcare-Associated Infections, Module I [Online]. Washington, D.C.: PAHO; [Published in December 2010, accessed in May 2023]. Available at: https://www.paho.org/es/documentos/modulo-i-vigilancia-epidemiologica-infecciones-asociadas-atencion-salud-2011
4.World Health Organization. Pan American Health Organization. Epidemiological Surveillance of Healthcare-Associated Infections, Module III [Online]. Washington, D.C.: PAHO; [Published in 2012, accessed in May 2023]. Available at: https://iris.paho.org/handle/10665.2/3270
5.Ministry of Health. Undersecretariat of Prevention and Health Promotion. General Directorate of Epidemiology. Manual of Standardized Procedures for Hospital Epidemiological Surveillance [Online]. Mexico: SSA; [Published in 2016, accessed May 2023]. Available at: https://epidemiologia.salud.gob.mx/gobmx/salud/documentos/manuales/28_Manual_RHoVE.pdf
6.Prevention and Health Promotion. General Directorate of Epidemiology. Epidemiological Overview of Healthcare-Associated Infections (HAIs) [Online]. Mexico: SSA; [Published in August 2022, accessed May 2023]. Available at: BOLETINRHOVECIERRE2022_FINAL.pdf (www.gob.mx)
7.Mexican Social Security Institute. Brief Guide for Epidemiological Surveillance, Prevention and Control of Healthcare-Associated Infections [Online]. Mexico: IMSS; [Published in December 2021, accessed in May 2022]. Available from: IMSS Website
8.Velázquez Mendoza J. Dolores, García Celedón Sergio Hugo, Velázquez Morales César Augusto, Vázquez Guerrero Miguel Ángel, Vega Malagón Alfredo Jesús. Prevalence of surgical site infection in patients undergoing abdominal surgery. Cir. gen [Online]. [Published in March 2011, accessed in May 2023]; 33(1): 32-37. Available from: http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S1405-00992011000100006&lng=es
9.Agreement number ACDO.AS3.HCT.251121/301.P.DF. Official Gazette of the Federation [Online]. Accessed May 2023. Available at: https://dof.gob.mx/nota_detalle.php?codigo=5639077&fecha=22/12/2021#gsc.tab=0
10.World Health Organization. WHO Global Guidelines for the Prevention of Surgical Site Infections. WHO; [Published December 15, 2016, accessed May 2023]. Available at: https://solucionesdesinfeccion.com/2016/12/15/guia-global-de-la-oms-para-la-prevencion-de-la-infeccion-de-herida-quirurgica/
11.World Health Organization. WHO recommends 29 ways to stop surgical site infections and prevent multidrug-resistant organisms. Press release [Online]. Geneva: WHO; [Published on 3 November 2016, accessed in May 2023]. Available at: https://www.who.int/es/news/item/03-11-2016-who-recommends-29-ways-to-stop-surgical-infections-and-avoid superbugs
12.Guanche Garcell H, Pérez Díaz CR, González Valdés A, Pisonero Socías JJ. Patient participation in the prevention of surgical site infections. Cuban Journal of Surgery [Online]. [Published April 2019, accessed May 2023];58(2):1–9. Available from: https://libcon.rec.uabc.mx:5471/login.aspx?direct=true&db=lth&AN=139204871&lang=es&site=ehost-live
13.Orozco HGH, Narváez JLC. Infection prevention. A look at the new “Global Guidelines for the Prevention of Surgical Site Infections.” Mexican Pediatric Journal [Online]. [Published January 2017, accessed May 2023];38(1):1–9. Available at: https://libcon.rec.uabc.mx:5471/login.aspx?direct=true&db=lth&AN=160265689&lang=es&site=ehost-live
14.Union of Deputies of the HC of the. Regulations of the General Health Law Regarding Health Research. General Health Law [Online]. 1987; DOF 02-04-:1–31. Available at: http://www.cofepris.gob.mx/MJ/Paginas/Reglamentos.aspx
15.National Commission for the Protection of Human Rights in Biomedical and Behavioral Research. Belmont Report: Ethical Principles and Guidelines for the Protection of Human Research Subjects. National Institutes of Health [Online]. 2003;12. Available at: https://www.etsu.edu/irb/Belmont Report in Spanish.pdf
16.Peñuela Epalza ME, Castro Silvera LM, Uricochea-Santiago AP, Díaz-Duque OL, Berdejo-Nieves JA, Silva-Gómez SE, et al. Risk factors for surgical site infection after appendectomy. A case-control study. Rev Salud Uninorte. [Published April 2018, accessed November 2023]; 34(1):97-108.
17.Fernández López O, Rodríguez Fernández Z, Ochoa Maren G, Pineda Chacón J, Romero García LI. Risk factors related to postoperative infections. [Published February 2016, accessed
18.Marycarmen Julissa Hidalgo-Costilla, Magdiel José Manuel Gonzales-Menéndez. Obesity as a factor associated with postoperative complications in patients undergoing abdominal surgery at the “Surgeon Major Santiago Tavara” Naval Medical Center during 2015. [Published in September 2017, accessed in November 2023] Available at: file:///C:/Users/quisq/Downloads/1194-Article%20Text-2554-3-10-20171218.pdf
19.García Díaz EDi. Diabetes mellitus as a risk factor for nosocomial surgical site infection in laparoscopic cholecystectomy. [Published on January 11, 2020, accessed in November 2023]; Available at: http://dspace.unitru.edu.pe/handle/UNITRU/11418
20.Ramos Beltrán C, Vargas Morales RE, Caballero Alvarado JA. Multivariate study of factors associated with surgical site infection in patients with hip arthroplasty. HAMPI RUNA. [Published December 13, 2018, accessed November 2023];17(1):15-29
21.Velasco E, Santos-Thuler LC, Martins CA, Castro-Dias LM, Conalves VM: Risk factors for infectious complications after abdominal surgery for malignant disease. Am J Infect Control. [Published February 2016, accessed November 2023] 24:1-6
22.Figuerola-Tejerina A, Rodríguez-Caravaca G, Bustamante-Munguira J, María San Román-Montero J, Durán-Poveda M. Epidemiological surveillance and risk factors for surgical site infection in cardiac surgery: a prospective cohort study. Rev Esp Cardiol. [Published September 1, 2016, accessed November 2023]; 69(09):842–8
23.Jaime Ruiz Tovara,b, Josep M. Badi. Measures for the prevention of surgical site infection in abdominal surgery. A critical review of the evidence. [Published August 3, 2013, accessed November 2023]. Available at: https://www.elsevier.es/es-revista-cirugia-espanola-36-articulo-medidas-prevencion-infeccion-del-sitio-S0009739X13003485
24.VincentCh, Moorthy K, Sarker SK, Chang A, Darzi AW; Systems Approaches to Surgical Quality and Safety From Concept to Measurement; Ann Surg [Published April 2004, accessed November 2023]; 39(4): 475–482
25.Urcuhuaranga Lezama ER. Associated factors for surgical site infection in patients in the intensive care unit of the Hipólito Unanue National Hospital from January to July 2018. Univ Priv S Juan Baut [Internet]. [Published January 2019, accessed November 2023]
26.Toro J, Barrera Ó, Morales C. Clinical superiority of laparoscopic appendectomy over the open technique: slow adoption of a new standard of care? Rev Colomb Cir. [Published March 30, 2017, accessed November 2023];32:32–9
27.Alonso-García M, de-la-Morena JM, de-la-Peña E, Martínez-Hurtado J, Lucas WC, del-MoralLuque JA, et al. Incidence of surgical site infection in renal surgery. Effect of the adequacy of antibiotic prophylaxis. Prospective cohort study. Actas Urol Esp. [Published December 1, 2018, accessed November 2023];42(10):639–44
28.Varela JE, Wilson SE, Nguyen NT. Laparoscopic surgery significantly reduces surgical-site infections compared with open surgery. Surg Endosc. [Published February 1, 2010, accessed November 2023];24(2):270–6.
29.Rodrigues de Carvalho RL, Campos CC, De Castro Franco LM, De Mattia Rocha A, Falci Ercole F, Carvalho RLR de, et al. Incidence and risk factors for surgical site infection in general surgeries. Rev Lat Am Enfermagem [Internet]. [Published January 2017, accessed November 2023]; 25. Available from: https://www.scielo.br/j/rlae/a/N9R5ZvPR7wzwwgbjBwbqFvJ/?lang=en
30.Gallagher M, Jones DJ, Bell-Syer SV. Prophylactic antibiotics to prevent surgical site infection after breast cancer surgery. [Published September 26, 2019, accessed November 2023];(9). Available at: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD005360.pub5/full/es?highli+ghtAbstract=withdrawn%7Csite%7Cinfection%7Csurgery%7Cinfect%7Csurgery
31.Del Moral Luque, Checa-García A, López-Hualda Á, Villar-del-Campo MC, Martínez-Martín J, Moreno-Coronas FJ, et al. Appropriateness of antibiotic prophylaxis in knee arthroplasty and surgical site infection: a prospective cohort study. Rev Esp Cir Ortopédica Traumatol. [Published July 1, 2017, accessed November 2023]; 61(4):259–64
32.Cheng H, Chen BP-H, Soleas IM, Ferko NC, Cameron CG, Hinoul P. Prolonged Operative Duration Increases Risk of Surgical Site Infections: A Systematic Review. Surg Infect. [Published August 1, 2017, accessed November 2023];18(6):722–35. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5685201/
33.Gómez-Romero P, Cabrera-Jardines R, Díaz-Green E, Rodríguez-Weber FL. Perioperative glycemic control: its importance and relationship with postoperative complications. [Published November 2016, accessed November 2023] 32(6):661-667. Available at: https://www.medigraphic.com/pdfs/medintmex/mim-2016/mim166h.pdf
Citation
Padilla-Morán A. and Serrano-García EA, Main risk factors associated with surgical site infection in adult patients treated in a general surgery service, ERSJ 2026,1(4) 189-205
Academic Editor: Brenda Leticia Rocha Reyes Received: 2025-december-12 Revised: 2026-april-08 Accepted: 2026-april-10 Published: 2026-april-18