Risk factors associated with poor prognosis in patients with cervical cancer at General Hospital No. 46
Jesús Alfonso Hernández Martínez and Dulce Azahar Padilla Sánchez
Unidad Médica Familiar 46 Avenida Periférico Carlos Pellicer Cámara S/N Col. Casa Blanca 2ª Sección, Villahermosa, Tabasco, CP 86060. Email: alfonsohdzmtz@gmail.com
Abstract
Introduction: Cervical cancer is a global public health problem, being the fourth most common type of cancer among women with an incidence of 13.3 per 100,000 in 2020 and a high mortality rate, especially in low- and middle-income countries. However, the need to identify risk factors to improve the prognosis and management of cervical cancer is imperative.Objetive: To analyze the risk factors associated with poor prognosis in patients with cervical cancer at General Hospital No. 46 in Villahermosa, Tabasco.
Materials and methods: Observational and analytical study, retrospective cohort, carried out at the General Hospital of Zone No. 46, with a total of 76 patients with histopathological diagnosis of cervical cancer from 2018 to 2023, applying a consecutive non-probabilistic sampling, obtaining the data from the electronic records of the patients.
Results: Most patients were diagnosed at advanced stages, which was associated with a higher risk of death, metastasis, and cancer recurrence. Factors such as the number of miscarriages, the type of treatment received, and occupation were significantly related to prognosis, and patients who did not undergo surgery or who received only chemotherapy or radiotherapy had a worse clinical course, likely due to being at more advanced stages.
Conclusions: The clinical stage at diagnosis is a key factor in prognosis, and early surgical intervention can significantly improve survival. Furthermore, the need to strengthen screening programs, ensure access to timely treatment, and design more effective follow-up strategies to reduce the impact of this disease on the most vulnerable women is emphasized.
Keywords: Cervical cancer, risk factors, recurrence, poor prognosis.
INTRODUCTION
Cervical cancer (CC) remains a leading cause of morbidity and mortality in women worldwide, despite being largely preventable through screening and vaccination strategies. In 2020, an estimated 604,000 new cases and 342,000 deaths were reported, making it the fourth most common cancer in women and one of the deadliest in low- and middle-income settings, where approximately 85% of deaths occur (1,2). This pattern reflects persistent inequalities in access to early diagnosis, timely treatment, and continuity of clinical follow-up.
In Latin America, the burden of CC remains high due to gaps in screening programs, institutional difficulties in ensuring continuous follow-up, and sociocultural factors that limit women's participation in preventive services (3). In Mexico, CC remains one of the most frequent cancers, with incidence and mortality rates higher than those observed in high-income countries. In response to this situation, the country has implemented various strategies: human papillomavirus (HPV) vaccination campaigns, improved Pap smear coverage, incorporation of HPV testing as primary screening, and increased funding for cancer treatments by the public system (4–6). These interventions have led to improved survival rates, reaching 68.5% in patients treated through public programs between 2006 and 2014 (5). However, a large proportion of cases continue to be diagnosed at advanced stages, which directly influences recurrence, metastasis, and mortality.
The progression of cervical cancer results from a complex interaction between viral, biological, gynecological-obstetric, sociodemographic, and healthcare access factors. The clinical stage at diagnosis, traditionally classified using FIGO, has been recognized as one of the most robust predictors of prognosis (7). The impact of factors such as the type of treatment received, the presence of lymph node metastases, therapeutic adherence, and delays in initiating cancer treatment—a frequent problem in overburdened healthcare systems—has also been documented (8–10). Recent studies also show the influence of characteristics such as age, parity, number of miscarriages, occupation, and education level on the risk of tumor progression and poor clinical outcome (11,12).
In Mexico, institutional research from the Mexican Social Security Institute (IMSS) has highlighted additional challenges, including the fragmentation of clinical records, loss to follow-up, and diagnostic delays resulting from administrative, logistical, and technological limitations (13,14). Although the IMSS has an Institutional Cancer Registry (RIC), the need to improve data collection and quality has been noted to strengthen epidemiological surveillance and the planning of cancer strategies (14). Early access to diagnostic and treatment services is a key factor in prognosis. Delays between cytology, colposcopy, biopsy, and the start of treatment have been linked to a higher risk of tumor progression, recurrence, and mortality (9,10). In vulnerable populations, factors such as occupation, socioeconomic status, and geographic barriers also have an additional impact, which can limit the use of health services (12,15). This is particularly relevant in areas like southeastern Mexico, where the incidence of cervical cancer is higher than in other regions of the country and where structural challenges in healthcare persist.
The General Hospital No. 46 of the Mexican Social Security Institute (IMSS) in Villahermosa, Tabasco, serves a heterogeneous population, predominantly working, with sociodemographic profiles that can influence access to prevention and timely care services. In this context, identifying the factors associated with poor prognosis in cervical cancer (CaC) is crucial for developing clinical, administrative, and community interventions aimed at improving survival. Understanding which risk factors—clinical, sociodemographic, and therapeutic—are related to adverse outcomes will not only strengthen medical decision-making but also guide institutional policies that reduce mortality and ensure comprehensive and continuous follow-up.
Consequently, this study arises from the need to evaluate, from an epidemiological perspective, the elements that contribute to poor prognosis in a local cohort of patients with cervical cancer, thus contributing to the generation of contextualized evidence that responds to the real needs of the region and the healthcare system, and supporting the improvement of screening programs, early diagnosis, timely treatment, and clinical surveillance. The objective of the study is to analyze the risk factors associated with poor prognosis in patients with cervical cancer at General Hospital No. 46 in Villahermosa, Tabasco.
MATERIALS AND METHODS
The study was conducted at General Hospital No. 46 of the Mexican Social Security Institute (IMSS) in Tabasco. It employed a retrospective cohort observational design, covering patients with a first-time histopathological diagnosis of cervical cancer between January 1, 2018, and December 31, 2023 (with follow-up until June 30, 2025).
Eighty-four patients with a first-time histopathologically confirmed diagnosis of cervical cancer between January 1, 2018, and December 31, 2023, were included (this represents all patients with this diagnosis during the specified period). Female patients over 18 years of age who were IMSS beneficiaries and had a first-time histopathological diagnosis of cervical cancer issued by another healthcare institution or whose medical records were incomplete were excluded. The study was conducted at the IMSS General Hospital No. 46, located in Villahermosa, Tabasco. A 6.5-year follow-up period was established, beginning on January 1, 2018, and ending on December 31, 2023, for the cohort. However, individual patients will be followed until June 30, 2025. The study was approved by the local research committee.
For data collection in this research, secondary data analysis was used, based on information recorded in the medical records of patients with a first-time histopathologically confirmed diagnosis of cervical cancer.
Statistical analysis was performed using SPSS software, employing the chi-square test for qualitative values, as well as Cox proportional hazards, with 95% confidence intervals.
RESULTS
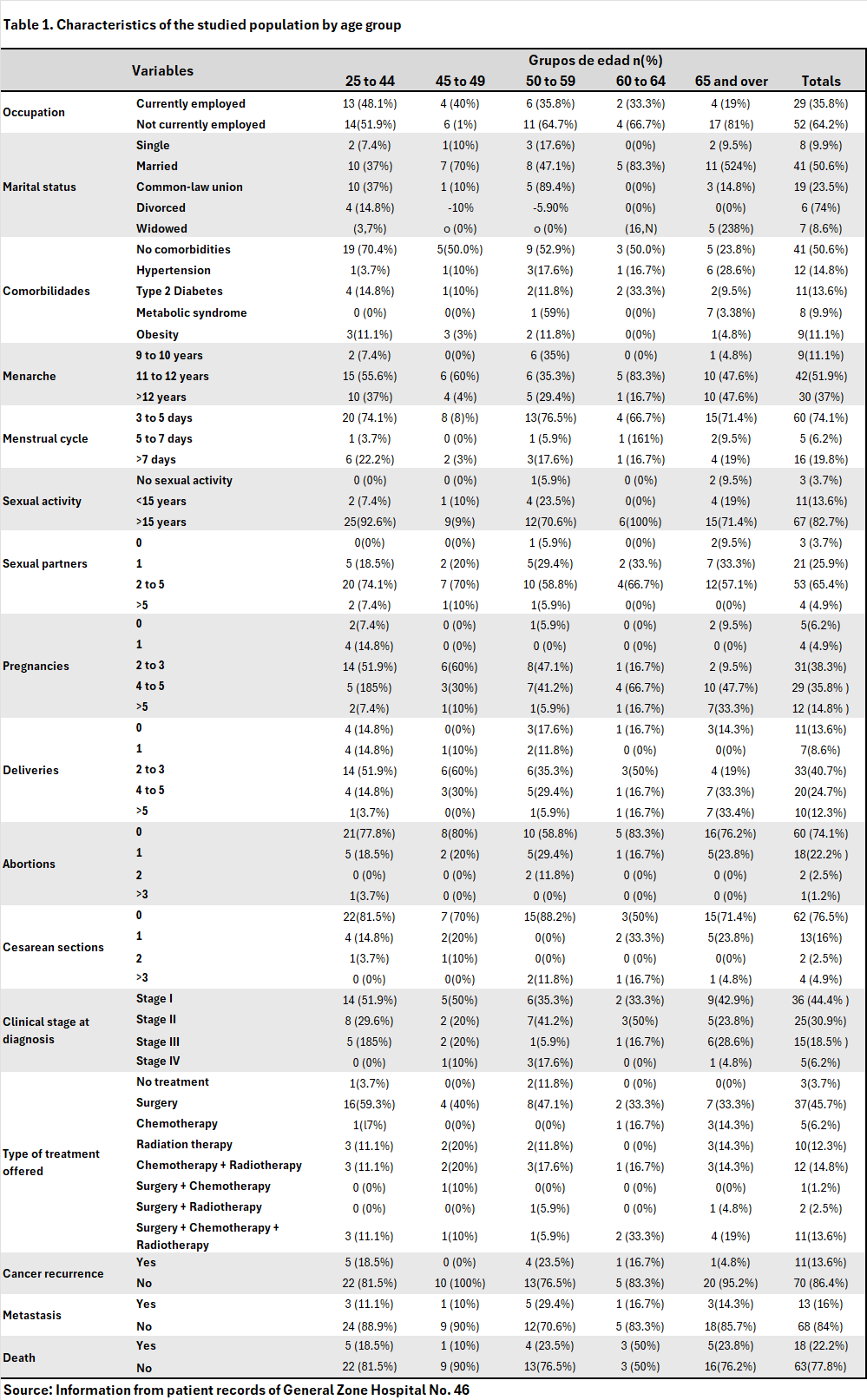
Eighty-one patients were included in the study, whose characteristics are described in Table 1.
The chi-square test was performed on the three outcome variables studied—Death, Recurrence, and Metastasis—against all covariates used in this study to assess whether there were significant differences between two categorical variables and to establish a relationship between them (Tables 2, 3, 4).
The relationship between occupational status and death was evaluated using a chi-square test. The results showed a statistically significant difference between the groups (χ² = 3.929; p = 0.047), suggesting that occupation may be associated with mortality in the analyzed population.
The chi-square test showed a statistically significant difference between the groups (χ² = 8.132; p = 0.043), suggesting a possible relationship between these variables within the analyzed sample. This finding indicates that the number of abortions may be associated with the occurrence of death.
The association between the variable “Clinical Stage at Diagnosis” and death was explored using the chi-square test. The results showed a statistically significant association between both variables (χ² = 22.661; p < 0.001), indicating that the proportion of deaths varies significantly among the different groups. These results suggest that this variable is strongly related to mortality in the studied population.
The relationship between having received surgical treatment and the occurrence of death was evaluated. The chi-square test showed a statistically significant difference between the two groups (χ² = 32.706; p < 0.001). This association suggests that patients who did not receive surgical treatment had a higher proportion of deaths compared to those who did.
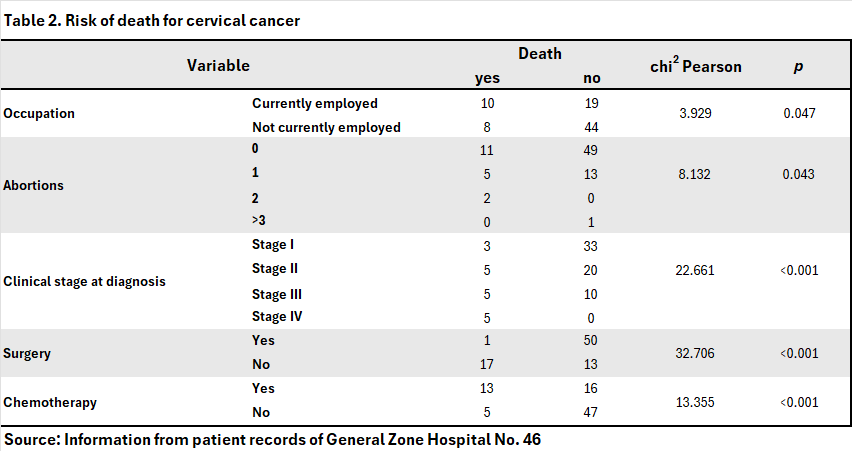
The possible association between having received chemotherapy treatment and the occurrence of death was analyzed. The chi-square test revealed a statistically significant association between the two variables (χ² = 13.355; p < 0.001). The data show that the proportion of deaths was considerably higher in the group that received chemotherapy compared to those who did not. This finding suggests that chemotherapy administration is associated with a higher risk of mortality in the studied population, which could be linked to the severity of the clinical condition of those who received this type of treatment.
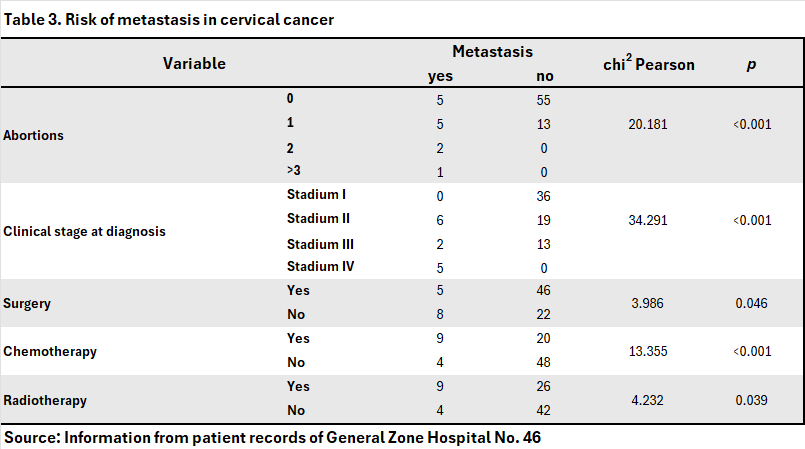
A significant association was found between the number of miscarriages and the presence of metastases (χ² = 20.181, p < 0.001). A higher number of miscarriages was associated with a higher frequency of metastases, although some categories had few cases.
A statistically significant association was identified between the clinical stage at the time of diagnosis and the presence of metastases (χ² = 34.291; p < 0.001). This indicates that the groups defined by this variable show notable differences in the proportions of metastases. A statistically significant association was found between having received surgical treatment and the presence of metastases (χ²=3.986; p=0.046). This suggests that patients who did not undergo surgery had a higher proportion of metastases compared to those who did.
A statistically significant association was observed between the administration of chemotherapy and the presence of metastases (χ²=13.355; p < 0.001), suggesting that chemotherapy may be related to a higher proportion of metastases.
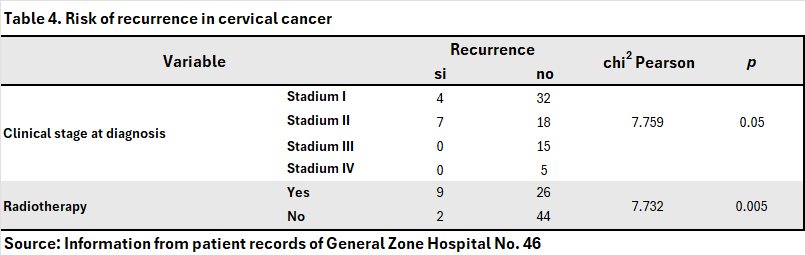
The chi-square test applied to evaluate the association between having received radiotherapy and the presence of metastases showed a statistically significant difference (χ²=4.273, p=0.039). This suggests that there is an association between radiotherapy treatment and the presence of metastases in the patients in the study. The relationship between the stage at diagnosis and the occurrence of cervical cancer recurrence was examined using the chi-square test. The results show a statistically significant difference between the analyzed groups (χ²=7.759; p=0.05). This suggests that the distribution of recurrences differs between Stages I, II, III, and IV.
When analyzing the relationship between having received radiotherapy and cervical cancer recurrence, a statistically significant association was found (χ²=7.732, p=0.005). This indicates that patients who received radiotherapy are statistically different from those who did not.
The mortality rate in this cohort was calculated by following our n (81) patients for a total of 389 person-years, of whom 19 died, yielding a rate of 48.84 deaths per 1,000 person-years.
The recurrence rate was estimated from the follow-up of 372 patients with a total of 11 recurrences, giving a rate of 29.57 recurrences per 1,000 person-years.
Finally, the metastasis rate was obtained by following 369 person-years, during which 13 patients developed metastases, resulting in a rate of 35.23 metastases per 1,000 person-years.
The estimated mean survival was 72.701 months, with a standard error of 3.459 months and a 95% confidence interval between 65.922 and 79.480 months. This figure reflects the average time that patients in the cohort lived from the start of follow-up until death or until the time of censoring, in the absence of other adjustment variables.
According to the Cox proportional hazards model results, the type of treatment received did not show a significant association with survival (HR=0.96; 95% CI: 0.78–1.19; p=0.709). In contrast, the clinical stage at diagnosis was a determining factor. Patients with more advanced stages had an almost three-fold increased risk of death (HR=2.898; 95% CI: 1.77–4.76; p < 0.001) compared to those with earlier stages.
The estimated median survival was 76,769 months, with a standard error of 3,203 months and a 95% confidence interval of 70,491 to 83,047 months. This figure reflects the average time patients in the cohort lived from the start of follow-up until the development of metastasis or until censoring, in the absence of other adjustment variables.
A Cox regression was performed to analyze the association between the type of treatment received and the clinical stage at diagnosis, along with the development of metastasis. The model is statistically significant overall (p < 0.001), indicating that the included variables (type of treatment and clinical stage at diagnosis) significantly contribute to explaining the risk of metastasis. Clinical stage at diagnosis acted as a powerful and independent predictor of metastasis risk. Patients in more advanced stages have an almost six-fold increased risk of developing metastases compared to those in early stages (HR = 5.841; 95% CI: 2.367–12.939; p < 0.001).
A final binary regression analysis was performed, identifying variables influential on the studied outcome of metastasis. Specifically, radiotherapy as the primary treatment and clinical stage at diagnosis showed statistically significant associations, suggesting their clinical relevance in the investigated context. The model suggests that the radiotherapy category was the only significant variable in the multivariate model (p = 0.007). The model explains between 12% and 21.9% of the variability in recurrence, representing low to moderate explanatory power. The non-significant value (p = 0.159) indicates that the model adequately fits the observed data.
The estimated mean survival was 80.391 months for recurrence, with a standard error of 2.516 months and a 95% confidence interval between 75.459 and 85.322 months. This figure reflects the average time that patients in the cohort lived from the start of follow-up until the onset of recurrence or until the time of censoring, in the absence of other adjustment variables.
A Cox regression was performed to analyze the association between the type of treatment received and the clinical stage at diagnosis with the occurrence of recurrence. The model is statistically significant overall (p=0.038), indicating that the variables of treatment type and clinical stage at diagnosis significantly contribute to explaining the risk of recurrence. Clinical stage at diagnosis acted as a strong and independent predictor of recurrence risk. Patients in more advanced stages had a 33.7% increased risk of recurrence compared to those in earlier stages (HR=1.337; 95% CI: 1.055–1.848; p=0.016), while the type of treatment was inconclusive.
DISCUSSION
The findings of this study, focused on the population of General Hospital Zone No. 46 in Villahermosa, Tabasco, reveal a complex reality regarding the risk factors that influence the poor prognosis of cervical cancer.
One of the most consistent findings in the reviewed literature, and one that this study confirms, is the strong association between advanced clinical stage at diagnosis and poor prognostic outcomes, such as death, recurrence, and metastasis. Jina Li et al. (2022) reported a significantly higher risk of recurrence in patients with stage II and higher, as well as worse long-term survival in those who experienced recurrence. Consistently, in this cohort, clinical stage was identified as a robust predictor of poor prognosis for all three outcomes analyzed. Cox proportional hazards models showed an exponential increase in the risk of death, metastasis, and recurrence as the disease progressed from stage I to stage IV, reinforcing the importance of timely diagnosis as a cornerstone of cervical cancer care.
Regarding recurrence, this study found a rate of 13.6%, with a mean recurrence rate of 2–3 years, in contrast to the 8% recurrence rate at five years reported by Jina Li et al. These differences may be due to the local healthcare context, treatment adherence, or variations in available therapeutic regimens, which also suggests an opportunity to improve postoperative follow-up and recurrence detection.
Concerning treatment, the results of Lambert Matos et al. (2021) in Cuba highlight the protective role of chemotherapy, while, paradoxically, this study found a statistically significant association between chemotherapy administration and a higher risk of death and metastasis. This apparent contradiction could be explained by indication bias; that is, the patients who received chemotherapy likely already had more advanced disease and, therefore, a guarded prognosis from the outset. In contrast, surgery showed a significant protective effect in our sample, a finding that aligns with studies such as the clinical trial by Plante et al. (2024), which showed good results with hysterectomy in early stages.
Likewise, the study by Linhares Moreira et al. (2020) also found that lymph node involvement and FIGO stage are determinants of the type and timing of recurrence. In this thesis, although lymph node involvement was not directly addressed, clinical stage again emerged as a fundamental prognostic factor, reinforcing its value as a clinical predictive tool.
Another relevant point was the association between the number of miscarriages and adverse outcomes, particularly metastasis. In this regard, the study by Jina Li et al. It was also reported that patients with three or more miscarriages had a 65% higher risk of recurrence, coinciding with the finding that this history negatively influences disease progression.
On the other hand, studies such as those by De Mey et al. (2021) highlight the role of radioresistance linked to genetic alterations such as BRCA1 and ATM. Although this study did not include molecular analysis, a statistically significant association was identified between radiotherapy treatment and a higher risk of recurrence and metastasis. This could be related to biological resistance to the treatment, although, as with chemotherapy, it could also reflect cases in more advanced stages with a worse baseline prognosis. However, this cannot be confirmed, since this study did not specifically target radioresistance.
Regarding sociodemographic factors, our findings coincide with the studies by Mpachika-Mfipa et al. (2019) and Gates et al. (2021), who documented that advanced age, low educational level, and marital status negatively influence access to screening and, therefore, timely detection. In this study, a large proportion of patients did not have completed their studies, and many were not in the workforce, which may reflect difficulties in accessing preventive services, also coinciding with the pattern observed in Mexico by Terán Figueroa et al. (2018), where household occupation and lack of contraceptive methods were related to a higher risk of mortality.
Finally, although immunotherapy was not part of this study, research such as that by Dyer et al. (2019) underscores the potential of targeted therapies to improve the prognosis of recurrent or metastatic cervical cancer. While these therapies are not yet available through the Mexican public healthcare system, they represent a future avenue for improving outcomes in advanced cases.
This study comprehensively analyzed the risk factors associated with poor prognosis in patients with cervical cancer treated at General Hospital No. 46 in Villahermosa, Tabasco. Using a quantitative approach, the sociodemographic and clinical characteristics of the cohort were examined, identifying specific profiles that provide valuable information about the evolution of this disease in the local (state) context.
It was found that most patients were of working age, with a low level of education and a high rate of unemployment, which can represent a barrier to timely access to healthcare services. Clinically, early-stage diagnosis predominated; however, failure to identify cervical cancer promptly was significantly associated with a higher probability of death, metastasis, and recurrence. This finding highlights the importance of early diagnosis as a determining factor in patient prognosis.
When adverse outcome rates were established, a mortality rate of 48.84 per 1,000 person-years, a recurrence rate of 29.57 per 1,000 person-years, and a metastasis rate of 35.23 per 1,000 person-years were observed, underscoring the clinical burden of this disease even after initial treatment.
Statistical analysis revealed that variables such as clinical stage at diagnosis, occupation, type of therapy offered, and especially access to surgical treatment, influence a good prognosis. Conversely, radiotherapy and chemotherapy without surgical treatment showed significant associations with negative outcomes, along with a history of three or more miscarriages. Notably, patients who did not receive surgery had higher rates of mortality and metastasis, while chemotherapy and radiotherapy, frequently indicated in advanced stages, were associated with a worse prognosis, possibly due to the severity of the disease at the time of treatment initiation.
Finally, these findings reinforce the need for public health strategies focused on early detection, equitable access to comprehensive treatments, and close follow-up of patients with cervical cancer, particularly in areas with limited infrastructure. Identifying these factors not only contributes to understanding the clinical behavior of the disease but also lays the groundwork for interventions aimed at improving the survival and quality of life of affected women.
REFERENCES
1.Globocan. Global Cancer Observatory. Cancer Today 2020. Available at: https://gco.iarc.fr/.
2.Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R. Cancer of the cervix: 2021 update. Int J Gynecol Obstet. 2021;155(S1):28–44.
3.De P, Public Health. Global strategy to accelerate the elimination of cervical cancer as a public health problem. WHO; 2020.
4.Ministry of Health. Specific Action Program for the Prevention and Control of Cancer in Women 2013–2018.
5.Torreglosa-Hernández S, et al. Survival analysis and associated factors in patients with cervical cancer financed by public funds in Mexico. BMC Cancer. 2022.
6.IMSS. Epidemiological Bulletin. 2023.
7.FIGO Committee on Gynecologic Oncology. Staging classification for cervical cancer. Int J Gynecol Obstet. 2019.
8.Ji M, Liu Y, Hu Y, et al. Comparison of recurrence patterns in cervical cancer patients with positive versus negative lymph nodes. Cancer Med. 2023;12(1):306–14.
9.Ferreira da Silva I, Koifman RJ. Cervical cancer treatment delays and associated factors in a developing country. J Glob Oncol. 2019.
10.Moreira ASL, Cunha TM, Esteves S. Cervical cancer recurrence – can we predict the type of recurrence? Radiol Interv Diag. 2020;26(5):403–10.
11.Li J, Liu G, Luo J, et al. Cervical cancer prognosis and related risk factors: a long-term retrospective cohort study. Sci Rep. 2022;12:17733.
12.Mpachika-Mfipa F, Kululanga LI, Kazembe A, Mfipa D. Sociodemographic determinants of cervical cancer screening uptake. BMC Cancer. 2022;22(1).
13.IMSS. Medical Indicators Portal. 2024.
14.Institutional Cancer Registry (RIC), IMSS.
15.Hernández-Hernández DM, Apresa-García T, Patlán-Pérez RM. Epidemiological overview of cervical cancer.2.
Citation
:Hernández Martínez JA and Padilla Sánchez DA, Risk factors associated with poor prognosis in patients with cervical cancer at General Hospital No. 46, ERSJ 2026,1(3) 143-154
Academic Editor: Alfonso Vallejos Paras, Received:07-November-2025, Revised:02-January-2026, Accepted:02-January-2026, Published:18-January-2026.