Comparison of the effectiveness of the BNT162b2 vaccine vs the ChAdOx1 vaccine in reducing the severity of COVID-19
Hernández-Peralta Efraín and Ruiz-Valdez Carmen Alicia
Instituto Mexicano del Seguro Social. Hospital General Regional No.1, Av. Vicente Guerrero, Bellavista, 85110, Obregón, Sonora, México
Abstract
Introduction: One of the challenges posed by the COVID-19 pandemic was the early development of a vaccine to reduce the severity of the disease. In Mexico, more than nine vaccines from different laboratories have been used; eventually, it will be necessary to continue acquiring batches only from laboratories whose vaccines have demonstrated the greatest effectiveness in the Mexican population.Objetive: To determine which of the BNT162b2 and ChAdOx1 nCoV-19 vaccines is more effective in reducing the severity of COVID-19.
Materials and methods: A cross-sectional, retrospective, analytical, observational study was conducted on the severity of COVID-19 in two groups of patients: one previously immunized with the BNT162b2 vaccine and the other with ChAdOx1, both treated at Regional General Hospital No. 1 in Ciudad Obregón, Sonora.
Results: Of the patients who developed severe illness, the largest proportion was in the group immunized with ChAdOx1 nCoV-19; this difference was statistically significant (p=0.03). Significant differences were also found in the frequency of pneumonia, Intensive Care Unit admission, and prolonged hospital stay.
Conclusions: Our study suggests that the BNT162b2 vaccine is more effective in preventing severe COVID-19 than the ChAdOx1 nCoV-19 vaccine.
Keywords: COVID-19, severe illness, effectiveness, BNT162b2, ChAdOx1 nCoV-19.
INTRODUCTION
The SARS-CoV-2 coronavirus has caused widespread economic and social devastation globally, and countries are engaged in an unprecedented vaccination campaign to contain it. By the end of 2021, 23 COVID-19 vaccines had been approved worldwide, exhibiting varying levels of efficacy, safety, and cost. 1
Eight COVID-19 vaccines have been authorized for emergency use in Mexico; however, studies of these vaccines in the Mexican population are still inconclusive. In this unprecedented pandemic, it is essential to have short- and medium-term information on the effectiveness of these vaccines in our population to guide public health decisions. 2,3
Since the emergence of the coronavirus, documented cases of COVID-19 have reached approximately 247 million worldwide, and recorded deaths exceeded 5 million by October 2021. Given this situation, it is not surprising that by early November 2021, the WHO had authorized the emergency use of up to seven COVID-19 vaccines.4,5,6
The development of COVID-19 vaccines and their mass application in less than two years since the emergence of this new pathogen has opened the possibility of achieving control of this pandemic. However, the reported effectiveness of the two vaccines mentioned has varied.15
The BNT162b2 COVID-19 vaccine is an mRNA-based vaccine produced by Pfizer Inc. and BioNTech; the ChAdOx1 nCoV-19 vaccine is a vaccine based on a replication-deficient simian adenovirus vector from the University of Oxford and AstraZeneca. Both contain nucleic acid that encodes the surface glycoprotein (spike protein) of SARS-CoV-2.8
Two doses of BNT162b2 are 95% effective (95% CI 90–98) at least 7 days after the second dose against symptomatic infection. In early 2021, research reported that BNT162b2 was 73% effective (95% CI: 62–82) 21–27 days after the first dose against symptomatic disease in people aged 70 years and older in Israel. After two doses, ChAdOx1 nCoV-19 has an efficacy of 70% against symptomatic infection.9,10,11
In a case-control study in England, the results show a relative risk of hospitalization of 0.57 (95% CI 0.48–0.67) for BNT162b2 and 0.63 (95% CI 0.41–0.97) for ChAdOx1 nCoV-19. In a study in Canada, the vaccine effectiveness against severe outcomes after 1 dose of BNT162b2 and ChAdOx1 nCoV-19 was 78% (95% CI, 65-86%) and 88% (95% CI, 60-96%), respectively.8, 12
An Israeli case-control study found that the estimated effectiveness of BNT162b2 against symptomatic disease in adults aged at least 70 years was 44% (95% CI: 49-64) at 14-24 days post-dose and 64% (37-83) at 21-27 days post-dose. In the same cohort, one dose of BNT162b2 had an estimated effectiveness against hospitalization of 74% (95% CI: 56-86) at 14-24 days after the first dose and 78% (61-91%) at 21-27 days after the first dose.13
A relevant factor to consider is the possible greater effectiveness of the ChAdOx1 nCoV-19 vaccine in the Mexican population compared to other populations; Trials of the vaccine showed a 63.9% protection rate against symptomatic SARS-CoV-2 infections, while in the case of a Mexican national, its effectiveness is 90%, according to the director of the Center for Research on Infectious Diseases (CISEI) of the INSP.14 In this research, we will focus on the study of two of them, BNT162b2 and ChAdOx1 nCoV-19, since they are two of the vaccines that have been administered in the largest numbers to the Mexican population, and because they are among those with the highest reported effectiveness.7
MATERIALS AND METHODS
This was a cross-sectional, retrospective, analytical observational study conducted at the Mexican Social Security Institute's Regional General Hospital No. 1 in Ciudad Obregón, Sonora. The dependent variable was the severity of COVID-19, and the independent variables were the brand of COVID-19 vaccine, age, sex, occupation, and comorbidities.
Patients with a complete SARS-CoV-2 immunization schedule using either the BNT162b2 or ChAdOx1 nCoV-19 vaccines prior to having COVID-19 confirmed by SARS-CoV-2 RT-PCR or SARS-CoV-2 Rapid Antigen Test at the General Regional Hospital No. 1 of the Mexican Social Security Institute (IMSS), Ciudad Obregón, Sonora, from January 5, 2021, to January 5, 2022.
The sample size was calculated for two proportions, based on a patient population with an alpha of 0.05 and a statistical power of 80%, resulting in a minimum of 71 patients.
Data was obtained from the epidemiological surveillance system for viral respiratory diseases of the Ministry of Health, using the SINOLAVE platform during the study period. This study included a review of physical (medical notes) and electronic medical records, as well as epidemiological studies and notes on suspected COVID-19 cases at Regional General Hospital No. 1. Inclusion criteria were patients of both sexes, 18 years of age or older, who had received at least two doses of immunization with the BNT162b2 or ChAdOx1 nCoV-19 vaccine between 30 and 270 days prior to symptom onset. COVID-19 was confirmed by RT-PCR or Rapid Antigen Test, with samples taken within the first 7 days of symptom onset, and who were treated at Regional General Hospital No. 1 IMSS, Ciudad Obregón, Sonora.
Exclusion criteria were patients classified by clinical assessment, those under 18 years of age, those with a hospital stay of less than 24 hours, patients without a final classification on the SINOLAVE platform, and those whose second vaccine dose had been administered less than 30 days or more than 9 months prior to receiving medical attention.
The information was collected using a format specifically designed to gather research variables of interest. Microsoft Excel software was used for data collection, and SPSS software was used for analysis.
The Kolmogorov-Smirnov test was used to assess normality of distribution for the scale variables. Additionally, the Mann-Whitney U test was used to compare the age distribution between the two study groups.
Measures of central tendency and dispersion were calculated for the scale variables, and proportions were calculated for the categorical variables.
Pearson's chi-square test was used to determine if there were statistically significant differences in the frequency of comorbidities and complications between the two groups.
To evaluate the association between vaccine brand and disease severity, odds ratios (OR) with 95% confidence intervals (95% CI) were calculated. A p-value of 0.05 or less was considered statistically significant.
The research was authorized by the local health research committee. It was considered to be of minimal risk because the studies used data risk in common procedures, in psychological or physical examinations for diagnosis or treatment.
RESULTS
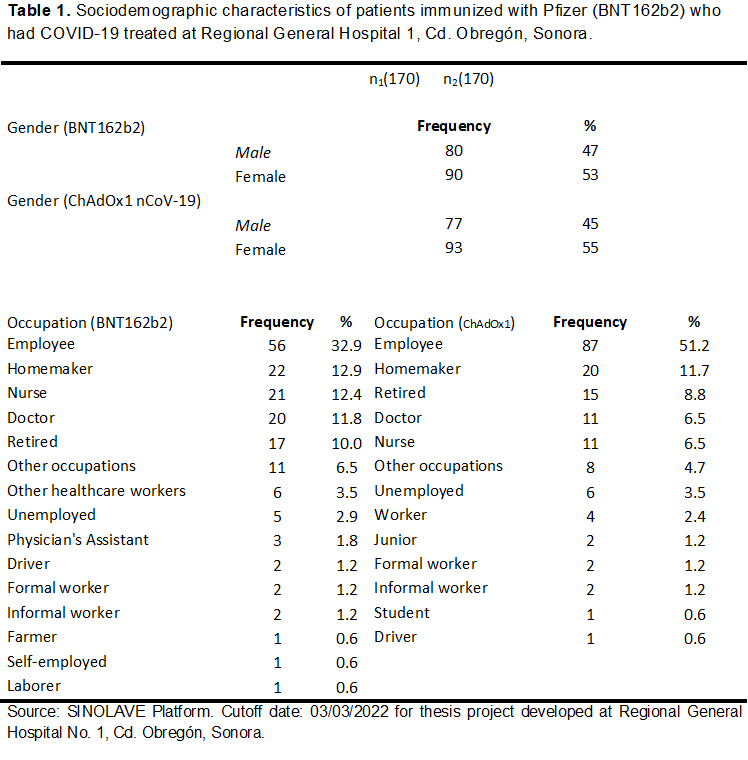
A total of 340 patients diagnosed with and confirmed to have COVID-19 at the General Regional Hospital No. 1, Ciudad Obregón, Sonora, were studied. They were divided into two groups of 170 subjects each, depending on the brand of COVID-19 vaccine with which they were immunized. In both groups, females were more frequent: 90 (53%) in the BNT162b2 group and 93 (55%) in the ChAdOx1 nCoV-19 group; while males were more frequent, with 80 (47%) and 77 (45%) respectively (Table 1). The patients' ages ranged from 19 to 79 years, with a mean of 49.3 years ± 15.4. In the group immunized with BNT162b2, the mean age was 49.8 years (SD 15.3 years), while in the group immunized with ChAdOx1 nCoV-19, the mean age was 48.7 years (SD 15.5 years).
The main occupations in the Pfizer group were similar in both groups: in the Pfizer group, they were employees (33%), homemakers (13%), nurses (12%), physician (12%), and retired (10%). In the Astra group, there were: employees (51%), homemakers (12%), retired (9%), physicians (6%), and nurse (6%) (Table 1).
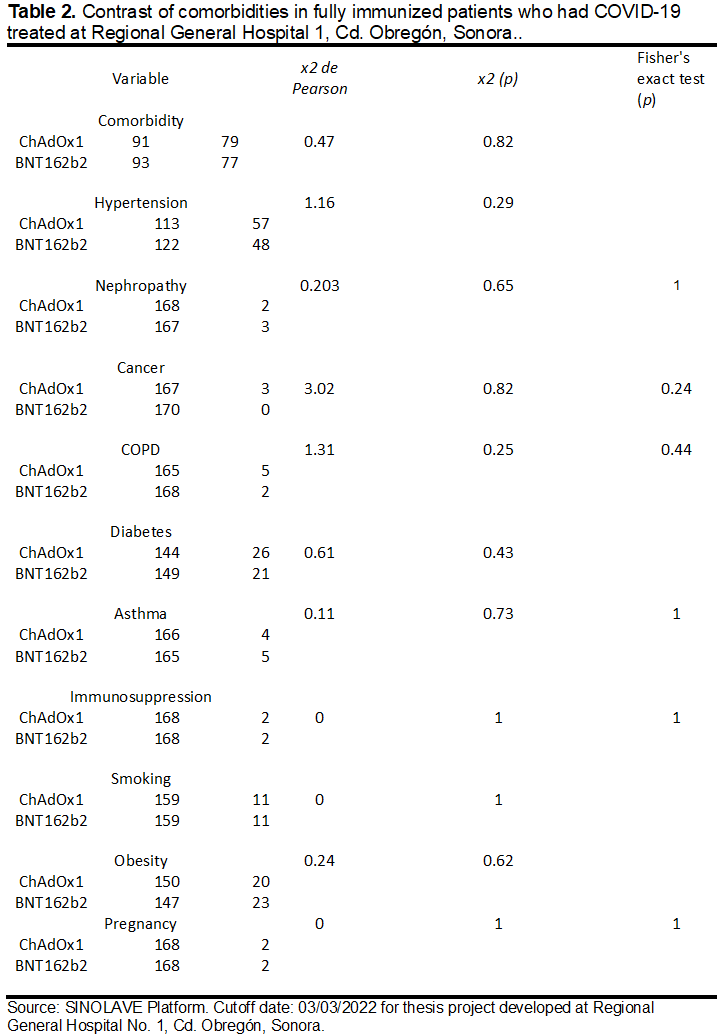
No statistically significant differences were found in the frequency of comorbidities between the two groups. Table 2 describes the proportions of each comorbidity, first for the BNT162b2 group and then for the Astra group, followed by the significance value of the Pearson chi-squared test. Hypertension 0.28 and 0.34 (p=0.29). Nephropathy 0.02 and 0.01 (p=0.65). Cancer 0 and 0.02 (p=0.08). COPD 0.01 and 0.03 (p=0.25). Diabetes mellitus 0.12 and 0.15 (p=0.43). Asthma 0.03 and 0.02 (p=0.73). Immunosuppression 0.01 and 0.01 (p=1). Smoking 0.06 and 0.05 (p=1). Obesity 0.14 and 0.12 (p=0.62). Pregnancy 0.01 and 0.01 (p=1).
No statistically significant differences were found between the two study groups for hospitalization, mechanical ventilation, or death (Table 3).
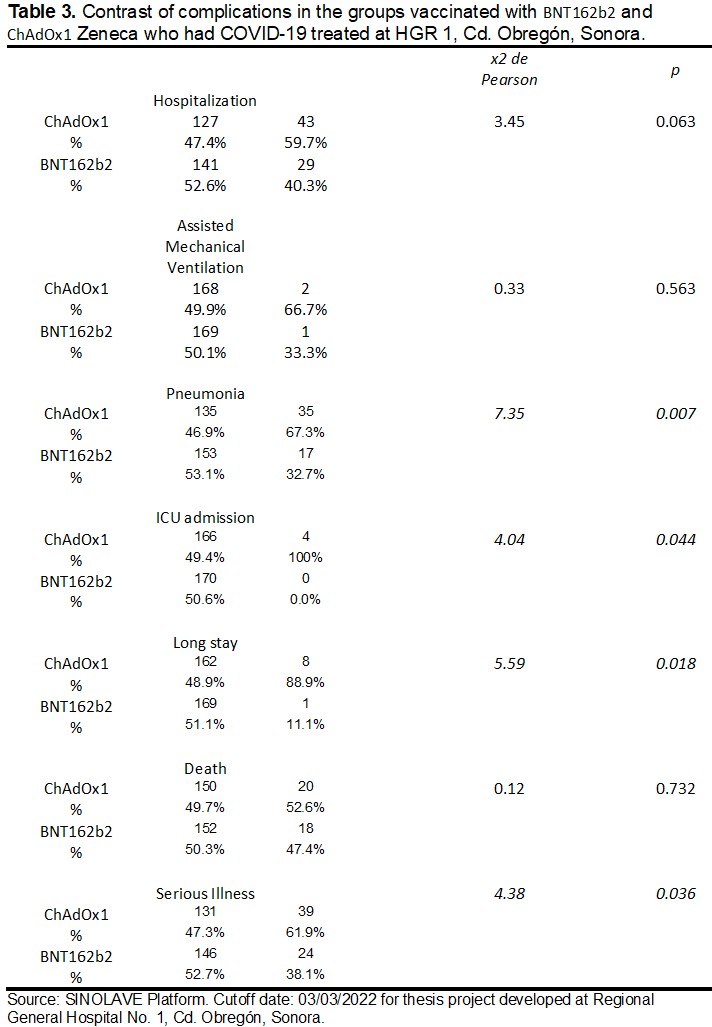
Among patients with pneumonia, 67.3% had been vaccinated with Astra and 32.7% with BNT162b2 (χ² test, p = 0.007, OR = 2.33, 95% CI: 1.2–4.35). None of the patients admitted to the ICU had a history of BNT162b2 vaccination; 100% had been immunized with ChAdOx1 nCoV-19 (χ² test, p = 0.044, OR = ∞) (Table 4).
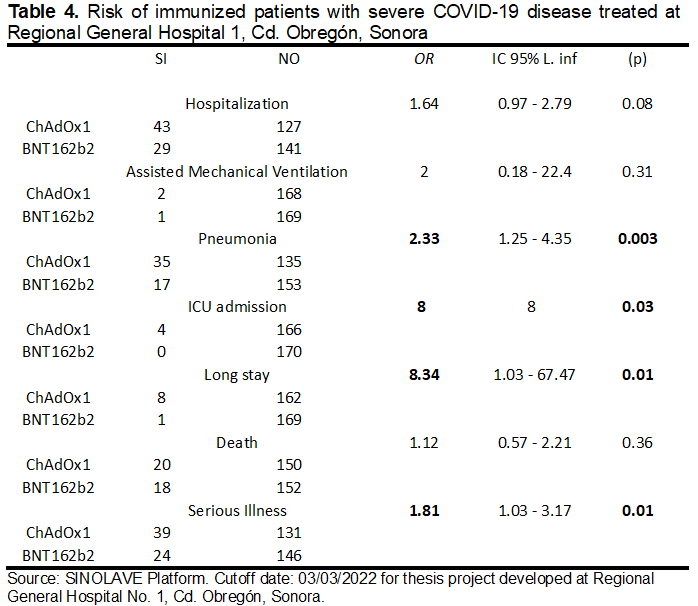
Prolonged hospital stays occurred in 9 patients, of whom 88.9% were immunized with Astra and 11.1% with BNT162b2 (χ² test, p=0.018; OR=8.34, 95% CI: 1.03-67.47). Severe disease occurred in 63 patients, of whom 61.9% were immunized with ChAdOx1 nCoV-19 and 38.1% with BNT162b2 (χ² test, p=0.036; OR=1.81, 95% CI: 1.02-2.57).
DISCUSSION
The complications of SARS-CoV-2 infection are heterogeneous and depend on multiple variables, such as age, sex, ethnicity, and comorbidities.20 In this study, both groups were homogeneous in age, gender, comorbidities, and occupation, so these factors did not affect the validity of the results.
Other authors have described that antibody concentrations increase more slowly and to a lower level with the ChAdOx1 nCoV-19 vaccine than with the BNT162b2 vaccine.21 This could also be a possible reason why severe illness occurred more frequently in the group vaccinated with ChAdOx1 nCoV-19.
In this study, no statistically significant differences were found between the two groups in terms of hospitalization risk reduction. International research differs on this point. While some authors found no difference between the two vaccine brands in reducing the risk of hospitalization,8 other studies describe differences in the hospitalization rate, with results favoring the BNT162b2 vaccine.22 This may be because hospitalization criteria vary significantly depending on geographic location, hospital unit, or even the stage of a COVID-19 wave, where factors such as the standard of care or bed availability can affect hospital admission thresholds.27
No greater benefit of one vaccine over the other was identified with respect to preventing death, which is consistent with what was described by Sheikh A. (2021), “the vaccine efficacy against death […] 14 days or more after the second dose of the vaccine, was 90% (95% CI, 83 to 94) for BNT162b2 and 91% (95% CI, 86 to 94) for ChAdOx1 nCoV-19”.25 These results should be interpreted with caution because death may not be a specific consequence of SARS-CoV-2 infection, especially during the Omicron variant wave, which had high infection rates.
A possible misclassification of the cause of death should be considered, particularly among older adults with comorbidities who are at higher risk of dying from other causes.27 When analyzing death as a complication, the cause of death should be validated as being due to COVID-19 and not merely associated with COVID-19.
The risk of requiring mechanical ventilation was similar in both groups; however, a significant difference (p=0.04) was found for ICU admission, favoring the BNT162b2 group. In the international literature, the reported effectiveness of ChAdOx1 nCoV-19 in preventing ICU admission was 89.9%, and in reducing the need for mechanical ventilation (MV) by 96.5%;23 while the effectiveness of BNT162b2 was 98% against ICU admission and the need for MV in a case-control study,24 however, a double-blind, randomized, placebo-controlled trial reported 100% effectiveness of ChAdOx1 nCoV-19 in preventing ICU admission.
A significant difference was found in favor of the BNT162b2 vaccine in the occurrence of pneumonia, OR=2.33 (p=0.003). No data were found in the international literature on the effectiveness of vaccines in reducing the risk of pneumonia; this could be because pneumonia is not traditionally considered a criterion for defining severe COVID-19. It is also possible to make the mistake of assuming that a hospitalized patient inherently has some degree of pneumonia, and therefore it is not studied as a complication. However, this is not always the case. In fact, many patients with confirmed COVID-19 may be hospitalized for non-respiratory reasons, and some who are present with respiratory symptoms may never develop pneumonia. For this reason, pneumonia, whether clinically defined or confirmed by laboratory testing, should be considered a complication or a criterion for defining severe COVID-19.
Among the complications studied in this research, prolonged hospital stay showed the highest odds ratio (OR) = 8.34 (p = 0.01) in favor of the BNT162b2 vaccine. Considering that both study groups were homogeneous with respect to sex, age, comorbidities, and occupation, we consider it unlikely that this difference is not due to the vaccine brand.
This research has some limitations. One of them is that the effectiveness reported in clinical trials of the BNT162b2 and ChAdOx1 nCoV-19 vaccines is expressed as a percentage obtained from the relative risk calculation, where it was possible to calculate the incidence of severe disease in immunized subjects versus non-immunized subjects. Our study is similar to a case-control study, so the effectiveness analysis is performed by calculating the odds ratio of subjects immunized with one brand versus subjects immunized with another brand. This creates a limitation if a direct comparison of effectiveness with international literature is intended; however, the main objective of the research is achieved.
According to the information analyzed in this study, severe COVID-19 occurred less frequently in the group of patients immunized with BNT162b2 compared to the group of patients immunized with ChAdOx1 nCoV-19. This difference was statistically significant, thus allowing us to answer the researcher's questions and accept the working hypothesis. This finding raises concerns about whether the effectiveness of the ChAdOx1 nCoV-19 vaccine in preventing severe COVID-19 is truly as reported by the Oxford-AstraZeneca laboratory. According to official reports, it should have similar results to the Pfizer vaccine; however, the results of this study suggest it is much lower, creating a precedent for larger, more controlled studies to clarify this issue and inform future COVID-19 vaccination policies in Mexico.
A slight predominance of females was found in both groups, although this difference was not statistically significant. The mean age, standard deviation, and age distribution were similar. Systemic hypertension and diabetes mellitus were the most frequent comorbidities in both groups. Thus, both groups were homogeneous in their sociodemographic and epidemiological characteristics.
One of the study's objectives was to quantify the magnitude of this difference. Finding that the risk of developing severe illness is 1.81 times higher when vaccinated with ChAdOx1 nCoV-19 compared to BNT162b2, this is an important finding as it contradicts official information on ChAdOx1 nCoV-19, which indicates that it has the same effectiveness as BNT162b2 in reducing the risk of severe COVID-19. This should be considered in public health decision-making regarding future contracts with laboratories.
When analyzing hospitalization rates between the two study groups, we found no statistically significant differences. However, when defining severe illness considering factors such as the need for mechanical ventilation, ICU admission, prolonged hospital stays, etc., we found significant differences between the two groups. This finding highlights the importance of following the current WHO recommendation not to consider hospitalization as the sole criterion for defining severe COVID-19 disease, but to use more specific definitions, since currently a large proportion of hospital admissions are associated with, but not caused by, SARS-CoV-2 infection, so these definitions probably better assess the protection of vaccines against COVID-19 disease.
REFERENCES
1. McGill Equipo de seguimiento de vacunas COVID19. “Vaccines candidates in clinical trials”. [en línea]. Montreal. COVID 19 Vaccine Tracker. [Actualizado: 05/11/2021, Consultado el: 07/11/2021]. Disponible en: https://covid19.trackvaccines.org/vaccines/
2. Secretaría de Salud de México. Resumen de las principales características de las vacunas disponibles en México. México. Portal Vacuna COVID del gobierno de México. Consultado el 03/11/2021. Disponible en: http://vacunacovid.gob.mx/wordpress/informacion-de-la-vacuna/
3. Ríos, Dulce Carolina, et al. "Vacunación por elección contra COVID-19 por la comunidad mexicana." Journal of Negative and No Positive Results 6.9 (2021): 1209-1221
4. Salud e Industria Farmaceutica. “Número de personas fallecidas a consecuencia del coronavirus a nivel mundial a fecha de 02 de noviembre de 2021, por continente”. [En línea]. Portal Statista. [Actualizado: 02/11/2021, Consultado: 09/11/2021]. Disponible en: https://es.statista.com/estadisticas/1107719/covid19-numero-de-muertes-a-nivel-mundial-por-region/
5. Organización Panamericana de la Salud. “Preguntas frecuentes: Vacunas contra la COVID-19.” [En línea]. Portal Vacunas contra COVID-19. [Actualizado: 11/03/2021, Consultado: 09/11/2021]. Disponible en: https://www.paho.org/es/vacunas-contra-covid-19/preguntas-frecuentes-vacunas-contra-covid-19
6. Asociación Mexicana de Industrias de Investigación Farmacéutica. “Estatus de las vacunas y ensayos clínicos para covid-19”. [En línea]. México. AMIF Innovación para la vida. [Actualizado: 04/11/2021, Consultado: 09/11/2021]. Disponible en: https://amiif.org/ya-se-habla-de-ensayos-clinicos-de-covid-19-sabes-lo-que-es-un-ensayo-clinico/
7. Salud e Industria Farmaceutica. “Número de dosis compradas de vacunas contra COVID-19 en México a 07 de noviembre de 2021, por tipo de vacuna”. [En línea]. Portal Statista. [Actualizado: 07/11/2021, Consultado: 09/11/2021]. Disponible en: https://es.statista.com/estadisticas/1207394/dosis-confirmadas-vacunas-covid-mexico/
8. Hyams, Catherine, et al. "Effectiveness of BNT162b2 and ChAdOx1 nCoV-19 COVID-19 vaccination at preventing hospitalisations in people aged at least 80 years: a test-negative, case-control study." The Lancet Infectious Diseases (2021).
9. Polack, Fernando P., et al. "Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine." New England Journal of Medicine (2020).
10. Dagan, Noa, et al. "BNT162b2 mRNA Covid-19 vaccine in a nationwide mass vaccination setting." New England Journal of Medicine 384.15 (2021): 1412-1423.
11. Voysey, Merryn, et al. "Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK." The Lancet 397.10269 (2021): 99-111.
12. Nasreen, Sharifa, et al. "Effectiveness of mRNA and ChAdOx1 COVID-19 vaccines against symptomatic SARS-CoV-2 infection and severe outcomes with variants of concern in Ontario”. Medrxiv (2021).
13. Dagan, Noa, et al. "BNT162b2 mRNA Covid-19 vaccine in a nationwide mass vaccination setting." New England Journal of Medicine 384.15 (20211): 1412-1423.
14. Revista Actualidad. “COVID-19: AstraZeneca con mayor efectividad en mexicanos: INSP”. [En línea]. Portal Revista Actualidad. [Actualizado: 15/08/2021, Consultado: 09/11/2021]. Disponible en: https://mexico.as.com/mexico/2021/08/16/actualidad/1629087507_235951.html
15. Noor, Rashed. "Developmental Status of the Potential Vaccines for the Mitigation of the COVID-19 Pandemic and a Focus on the Effectiveness of the Pfizer-BioNTech and Moderna mRNA Vaccines." Current clinical microbiology reports (2021): 1-8.
16. Glatman-Freedman, Aharona, et al. "The BNT162b2 vaccine effectiveness against new COVID-19 cases and complications of breakthrough cases: A nation-wide retrospective longitudinal multiple cohort analysis using individualised data." EBioMedicine 72 (2021): 103574.
17. Vaishya, Raju, et al. "Symptomatic post-vaccination SARS-CoV-2 infections in healthcare workers–A multicenter cohort study." Diabetes & Metabolic Syndrome: Clinical Research & Reviews 15.6 (2021): 102306.
18. Logunov, Denis Y., et al. "Safety and immunogenicity of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine in two formulations: two open, non-randomised phase 1/2 studies from Russia." The Lancet 396.10255 (2020): 887-897.
19. Grupo Técnico Asesor de Vacunación Covid. México. "Priorización inicial y consecutiva para la vacunación contra SARS-CoV-2 en la población mexicana. Recomendaciones preliminares." salud pública de méxico 63.2 (2021): 286-307.
20. Hodgson, Susanne H., et al. "What defines an efficacious COVID-19 vaccine? A review of the challenges assessing the clinical efficacy of vaccines against SARS-CoV-2." The lancet infectious diseases 21.2 (2021): e26-e35.
21. Lacobucci, G. (2021). Covid-19: Infections fell by 65% after first dose of AstraZeneca or Pfizer vaccine, data show. bmj, 373, n1068.
22. Bernal, J. L., Andrews, N., Gower, C., Robertson, C., Stowe, J., Tessier, E., .. & Ramsay, M. (2021). Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on covid-19 related symptoms, hospital admissions, and mortality in older adults in England: test negative case-control study. bmj, 373.
23. Hitchings, M. D., Ranzani, O. T., Dorion, M., D’Agostini, T. L., de Paula, R. C., de Paula, O. F. P., ... & Croda, J. (2021). Effectiveness of ChAdOx1 vaccine in older adults during SARS-CoV-2 Gamma variant circulation in São Paulo. Nature communications, 12(1), 1-8.
24. Olson, S. M., Newhams, M. M., Halasa, N. B., Price, A. M., Boom, J. A., Sahni, L. C., ... & Randolph, A. G. (2022). Effectiveness of BNT162b2 vaccine against critical Covid-19 in adolescents. New England Journal of Medicine, 386(8), 713-723.
25. Sheikh, A., Robertson, C., & Taylor, B. (2021). BNT162b2 and ChAdOx1 nCoV-19 vaccine effectiveness against death from the delta variant. New England Journal of Medicine, 385(23), 2195-2197.
26. Kaura, A., Trickey, A., Shah, A. S., Benedetto, U., Glampson, B., Mulla, A., ... & Mayet, J. (2022). Comparing the longer-term effectiveness of a single dose of the Pfizer-BioNTech and Oxford-AstraZeneca COVID-19 vaccines across the age spectrum. EClinicalMedicine, 46, 101344.
27. Feikin, D. R., Abu-Raddad, L. J., Andrews, N., Davies, M. A., Higdon, M. M., Orenstein, W. A., & Patel, M. K. (2022). Assessing vaccine effectiveness against severe COVID-19 disease caused by omicron variant. Report from a meeting of the World Health Organization. Vaccine, 40(26), 3516-3527.
28. Falsey, A. R., Sobieszczyk, M. E., Hirsch, I., Sproule, S., Robb, M. L., Corey, L., ... & Gonzalez-Lopez, A. (2021). Phase 3 safety and efficacy of AZD1222 (ChAdOx1 nCoV-19) Covid-19 vaccine. New England Journal of Medicine, 385(25), 2348-2360.
29. Higdon, M. M., Wahl, B., Jones, C. B., Rosen, J. G., Truelove, S. A., Baidya, A., ... & Hill, A. L. (2021, September). A systematic review of COVID-19 vaccine efficacy and effectiveness against SARS-CoV-2 infection and disease. In Open Forum Infectious Diseases.
Citation
Hernández-Peralta E and Ruiz-Valdez CA, Comparison of the effectiveness of the BNT162b2 vaccine vs the ChAdOx1 vaccine in reducing the severity of COVID-19, ERSJ 2026,1(3) 111-124
Academic Editor:Hernández Bautista Porfirio Felipe, Received:4-agosto-2025, Revised: 22-dicembre-2025, Accepted: 22 diciembre-2025, Published: 18-Enero -2026.