Complications associated with SARS-Cov-2 infection in hospitalized patients with diabetes mellitus
Juan Alberto Castillo-Chapa and Carmen Alicia Ruíz-Valdez
Instituto Mexicano del Seguro Social. Hospital General Regional No.1, Av. Vicente Guerrero, Bellavista, 85110, Obregón, Sonora, México
Abstract
Introduction: In populations where type 2 diabetes mellitus is a highly prevalent condition and adequate glycemic control is lacking, such as in Mexico, further investigation into its relationship with COVID-19 is warranted.Objetive: To identify complications associated with SARS-CoV2 infection in hospitalized patients with diabetes mellitus at IMSS Regional General Hospital No. 1, Ciudad Obregón, Sonora.
Materials and methods: A cross-sectional, observational, and descriptive clinical epidemiological study was conducted at the IMSS Regional General Hospital No. 1, Ciudad Obregón, Sonora, from March 23, 2020, to March 23, 2021.
Results: For the study, 286 patients were analyzed, organized into a study group (n = 176) and a control group (n = 110), using the Mann-Whitney U test, it was found that there is a relationship between Diabetes Mellitus and the appearance of complications (p = 0.002) such as pneumonia (p = 0.00002), severe acute respiratory syndrome (p = 0.0003) and death (p = 0.015). Hyperglycemia greater than 164 mg / dL is related to the appearance of complications (p = 0.001) and greater than 234 mg / dL is associated with death (p = 0.0003).
Conclusions: An association between complications and SARS-CoV-2 infection was identified in hospitalized patients with diabetes mellitus; based on the results, it can be inferred that these may apply to the general population. Glycemic control plays a key role in the development of complications, so glycemic control should be a cornerstone of COVID-19 treatment.
Keywords: Diabetes mellitus, complications, SARS-CoV2, COVID-19.
INTRODUCTION
Diabetes mellitus (DM) is a chronic-degenerative condition1 in which the pancreas is unable to synthesize insulin or occurs when the body is unable to use this hormone.2 In the long term, the resulting hyperglycemia can cause damage to various organs, causing serious complications, such as cardiovascular disease, increased susceptibility to infections 3 diabetic neuropathy, diabetic nephropathy, diabetic retinopathy, among others.4 The SARS-CoV-2 disease called COVID-19,8 is a disease9 that was identified after an outbreak of pneumonia of unknown etiology in Wuhan, China at the end of 2019;10 which on March 11, 2020 was declared a pandemic by the WHO,11 so that as of November 8, 2020, 49.7 million cases have been reported worldwide, with more than 1.2 million deaths associated with this disease since the beginning of the pandemic.12 As a result of this information, the identification of complications associated with SARS-CoV-2 infection in patients with diabetes mellitus, specifically in hospitalized patients, is considered relevant.
The SARS-CoV-2 virus, belonging to the Coronaviridae family,13 is a virus that contains a single strand of ribonucleic acid (RNA),14 whose family has the ability to infect humans, like those that cause Middle East Respiratory Syndrome (MERS-CoV) and Severe Acute Respiratory Syndrome (SARS-CoV),11 both with the ability to develop into epidemics.13 It has been studied that SARS-CoV2 has the ability to be transmitted from person to person through respiratory droplets,15 including transmission from asymptomatic cases,14 and due to the lack of treatment and specific prevention measures, it has become a major public health problem worldwide.11
Patients with COVID-19 disease usually present symptoms similar to a respiratory tract illness,8 the most common symptoms being fever and cough,9 as well as headache, dyspnea, myalgia, arthralgia, anosmia, dysgeusia, chest pain and, to a lesser extent, diarrhea and vomiting.11,14 The disease may not manifest itself, as in asymptomatic cases;15 and may also have a mild presentation with symptoms that do not endanger the patient's life8 or present with severe acute respiratory syndrome due to SARS-CoV-2, where the lung condition is severe,13 with an increase in cytokines and chemokines, known as a cytokine storm,5,9,16 which increases the proinflammatory state of patients.9,16
Multiple therapeutic trials have been carried out to try to identify an effective treatment against COVID-19, however these have been unsuccessful and there is no approved medication for its management,15 however it has been verified that the use of steroids has helped reduce mortality in hospitalized patients with invasive mechanical ventilation;17 Likewise, in order to better understand this new disease, certain conditions such as advanced age, presence of systemic arterial hypertension (SAH), obesity, chronic obstructive pulmonary disease (COPD), asthma, smoking and DM have been identified as risk factors associated with a worse prognosis,14 including death in patients with COVID-19.18
According to certain publications, it has been suggested that patients living with diabetes who develop COVID-19 present an inflammatory process enhanced18 by the pathophysiology of both diseases, in which an increase in blood glucose levels is observed secondary to the same inflammatory process.5,15,19 Therefore, there is a consequent high risk of complications secondary to SARS-CoV-2 infection such as pneumonia, severe acute respiratory syndrome, septic shock, acute kidney injury, multiorgan failure, or death.16,19,20
Due to the recent introduction of COVID-19 and the lack of understanding of it, it is important to continue studying SARS-CoV-2 infection, specifically in immunocompromised patients such as those living with diabetes, as well as its complications and possible risk factors.16
Therefore, in this study, we did not propose to identify complications associated with SARS-CoV-2 infection in hospitalized patients with diabetes mellitus.
MATERIALS AND METHODS
For the purpose of this research, a cross-sectional, descriptive, observational study was designed at IMSS Regional General Hospital No. 1 in Ciudad Obregón, Sonora. The study was conducted from March 23, 2020, to March 23, 2021.
Data were obtained through review of medical notes and clinical records during the study period. Data were supplemented with information from the laboratory results platform used at the same hospital and data obtained through the SINOLAVE platform.
Cases were confirmed with RT-PCR for COVID-19, reported by IMSS Regional General Hospital No. 1 in Ciudad Obregón, Sonora, during the study period, and information was available.
A sample size calculation was performed for a proportion of a finite population of confirmed COVID-19 cases using RT-PCR for SARS-CoV-2 at IMSS Regional General Hospital No. 1, Ciudad Obregón, Sonora, during the study period. The result was 225.
The independent variables were: pneumonia, severe acute respiratory syndrome, invasive mechanical ventilation, septic shock, acute kidney injury, multiple organ failure, tertiary referral, diabetes mellitus, blood glucose, glycemic control, confirmed COVID-19 case, age, gender, comorbidities, and the dependent variable was hospital discharge or death.
The inclusion criteria were: patients of both sexes, of any age, including pediatric patients, IMSS beneficiaries, patients considered confirmed cases of COVID-19, notified by IMSS Regional General Hospital No. 1, Ciudad Obregón, Sonora, and patients hospitalized at IMSS Regional General Hospital No. 1, Ciudad Obregón, Sonora.
The exclusion criteria were: patients referred to another secondary care hospital, with a record of pregnancy or postpartum, with a hospital stay of less than 24 hours, and with missing blood glucose or capillary glucose laboratory results in a medical note, clinical record, or on the laboratory platform.
The elimination criteria were: duplicate cases on the SINOLAVE platform, discharge for reasons other than improvement or death, death from causes not associated with COVID-19, incomplete data in medical notes, clinical records, the SINOLAVE platform, or the laboratory platform that prevented adequate data collection. The study was authorized by the local health research committee. The data was collected using a specially designed format, which allowed for the necessary information to be obtained, eliminating data that would identify the cases, thus ensuring patient anonymity and confidentiality.
Data were collected retrospectively from medical notes, clinical records, laboratory results issued by the same hospital's platform, and the institutional SINOLAVE platform, according to the calculated sample size. Data were entered into a database created with Excel version 365. Data analysis was performed using IBM SPSS version 24. Statistical tests were applied to perform univariate and bivariate analyses, using complications associated with SARS-CoV-2 infection as the dependent variable. Hypothesis testing was performed using the Mann-Whitney U test, the median test for independent samples, and Spearman's Rho. A p value < 0.05 was considered statistically significant.
RESULTS
Due to the number of reported cases, a sample of 286 patients was obtained, exceeding the sample calculated for greater statistical significance. Of these 286 cases, 176 with a history of DM and 110 without were selected, forming the study group (SG) and control group (CG), respectively.
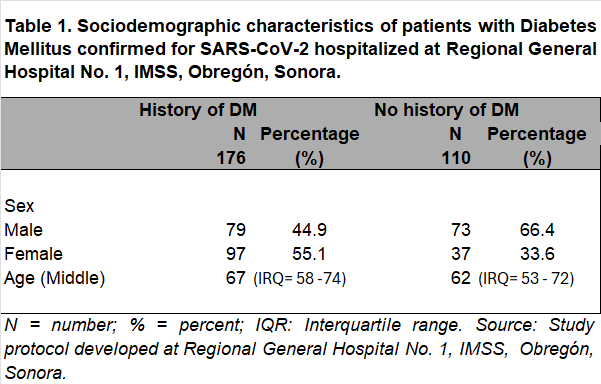
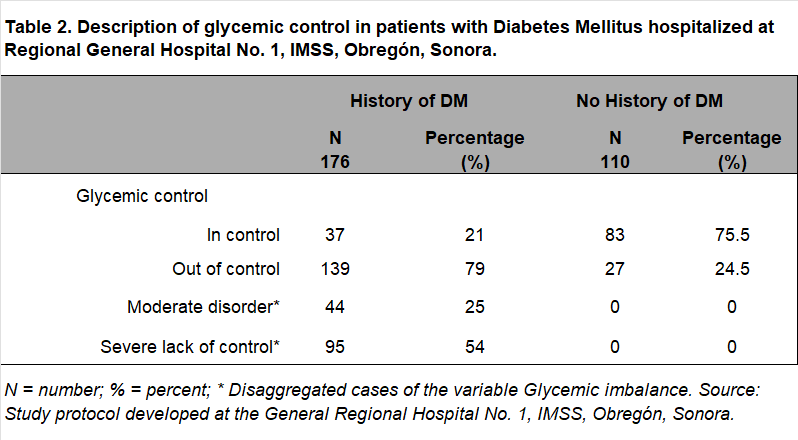
A total of 286 patients were analyzed as confirmed cases of COVID-19, of which 53.1% (n=152) were male and 46.9% (n=134) were female. Their ages ranged from 16 to 93 years, with a median age of 65 years (IQR=55–74). Of these patients, 176 had a history of DM and COVID-19, of whom 44.9% (n=79) were male and 55.1% (n=97) were female. Their ages ranged from 24 to 88 years, with a median age of 67 (IQR=58–74) (Table 1). Regarding glycemic control, it was found that, of the 176 patients in the EG, 21% (n=37) were controlled, while 78.9% (n=139) had glycemic dyscontrol; of the latter, 31.6% (n=44) were in moderate dyscontrol and 68.3% (n=95) in severe dyscontrol. A median glucose level of 232 mg/dL (IQR= 162–304) was identified in this group. In the CG, it was found that 75.5% (n=83) were in adequate glycemic control, while 24.5% (n=27) presented hyperglycemia (Table 2); this group presented a median glucose level of 128 mg/dL (IQR= 100–150).
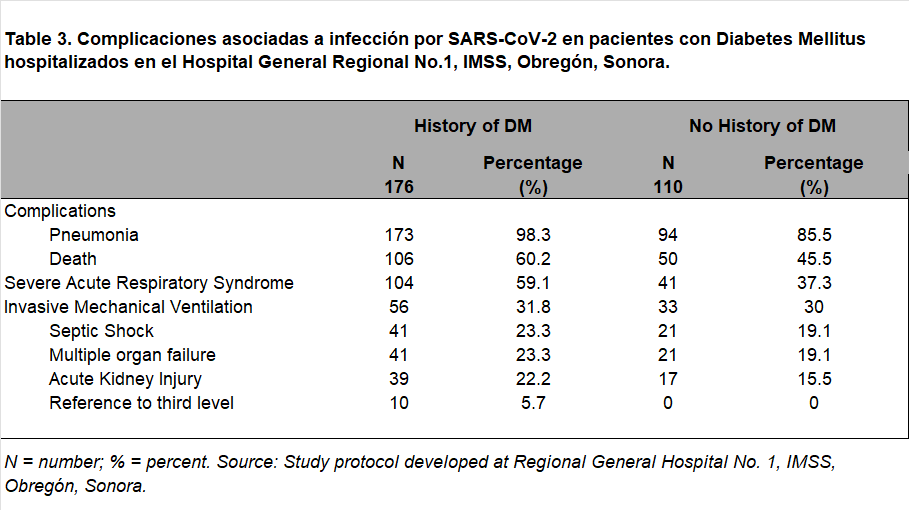
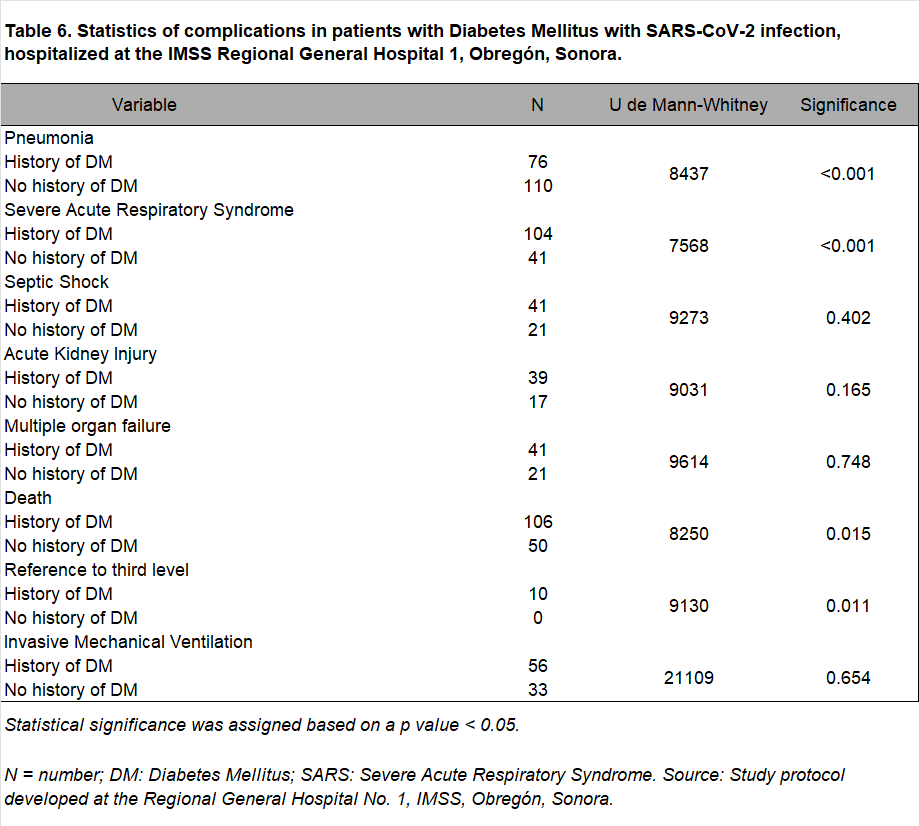
Regarding the reported complications, pneumonia was found in 98.3% of the study group (n=173), death in 60.2% (n=106), severe acute respiratory syndrome in 59.1% (n=104), requirement for invasive mechanical ventilation in 31.8% (n=56), septic shock and multiple organ failure in 23.3% (n=41) each, acute kidney injury in 22.2% (n=39) and referral to third level in 5.7% (n=10). In the control group, pneumonia was found in 85.5% (n=94), death in 45.5% (n=50), severe acute respiratory syndrome in 37.3% (n=41), invasive mechanical ventilation in 30% (n=30), septic shock and multiorgan failure in 19.1% (n=21) each, acute kidney injury in 15.5% (n=17), and no referrals to tertiary care were reported (Table 3).
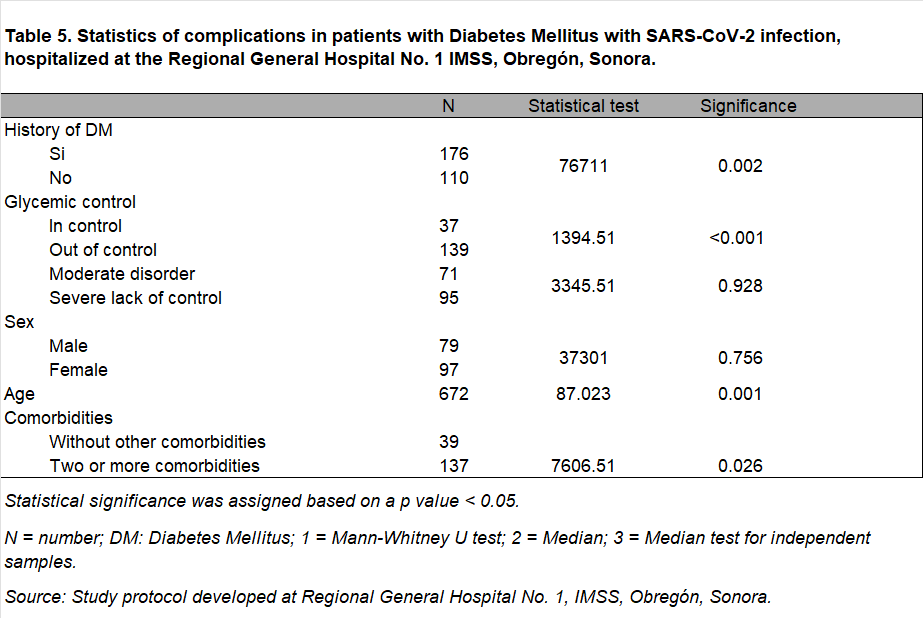
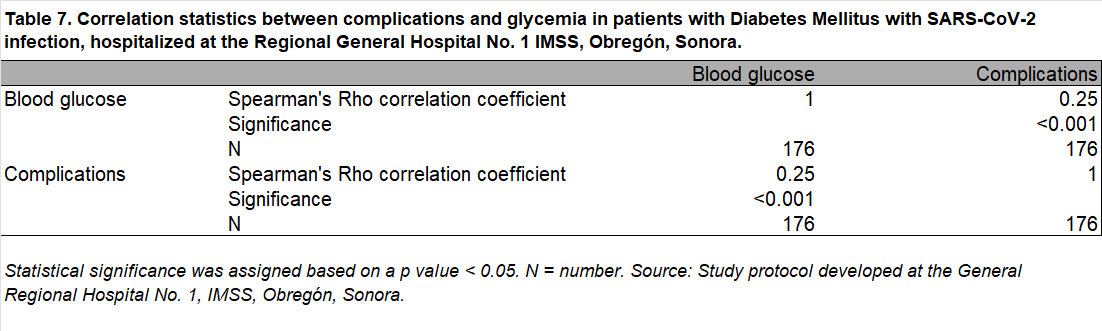
A statistically significant difference was found regarding the presence of complications in patients with diabetes and SARS-CoV-2 infection (p=0.002). It was also found that glycemic control was related to the development of complications (p=0.0001); however, there was no relationship between moderate and severe glycemic control (p=0.928) (Table 5). Age is associated with the presence of complications in these patients (p=0.0003). A history of DM is associated with the following complications: pneumonia in patients with SARS (p=0.0002), presence of SARS (p=0.003), referral to a third level (p=0.0004), and death (p=0.01). Furthermore, the latter is related to glycemic control (p=0.004) (Table 5 and Table 6). Gender is not associated with the occurrence of complications (p=0.756). Blood glucose levels (SD=164.5) and complications are associated (p=0.001) (Table 7), as is the case for blood glucose levels (SD=249.34). On the other hand, it was found that the presence of two comorbidities is associated with the appearance of complications in these patients (p= 0.045) (Table 5).
DISCUSSION
Due to the evolution of the COVID-19 pandemic and the clinical relevance of this disease, numerous but insufficient research studies have emerged to determine risk factors, prognostic factors, as well as clinical trials to evaluate treatments and even vaccine safety studies that allow mitigating and controlling the pandemic.
Accordingly, it was important to identify the complications associated with SARS-CoV-2 infection in hospitalized patients with Diabetes Mellitus at the IMSS Regional General Hospital No. 1, Ciudad Obregón, Sonora, as the main objective of this research work. Therefore, by obtaining a significant sample, it was possible to achieve statistical significance and internal and external validity in this research work. After conducting the study, it was found that the main complications in patients living with DM who are hospitalized after SARS-CoV-2 infection are pneumonia, death, and severe acute respiratory syndrome. Likewise, it was found that there is a relationship between the presence of Diabetes Mellitus and the development of complications in these same patients with COVID-19, which is consistent with studies conducted by Huang I et al.18
For the variables septic shock, acute kidney injury, multiple organ failure, and the need for invasive mechanical ventilation, no statistically significant relationship was found; therefore, it is advisable to continue searching for the factors that influence the development and prevention of these complications.
It is important to note that social and demographic factors of the population do play an important role in the development of complications in these patients. This research protocol demonstrated that age is related to the development of complications; however, sex is not associated with their occurrence. According to the study "Coronavirus Infection in Patients with Diabetes" by Torres-Tamayo M. et al., the importance of advanced age is mentioned, considering it a promoter of morbidity and mortality in patients with DM and COVID-19.5
Regarding glycemic control, it was found that only 21% of patients with DM had blood glucose levels below 140 mg/dL, while 25% had moderate dyscontrol (140–199 mg/dL) and 53.9% had severe dyscontrol (greater than 200 mg/dL). Of these patients, 65.9% had more than two complications. In addition, it was observed that blood glucose levels above 164.5 mg/dL are related to the onset of complications and the need for management by a third level of medical care. Blood glucose levels above 234 mg/dL are associated with the variable death. According to Bellido V. in his research work, it is mentioned that hyperglycemia is related to a greater number of complications and an increase in mortality; however, the cut-off level for glucose they used was 180 mg/dL.6 According to this research work, there is no statistically significant difference between moderate and severe glycemic control, so it would be advisable to continue investigating this finding to dictate therapeutic guidelines and control goals in the future.
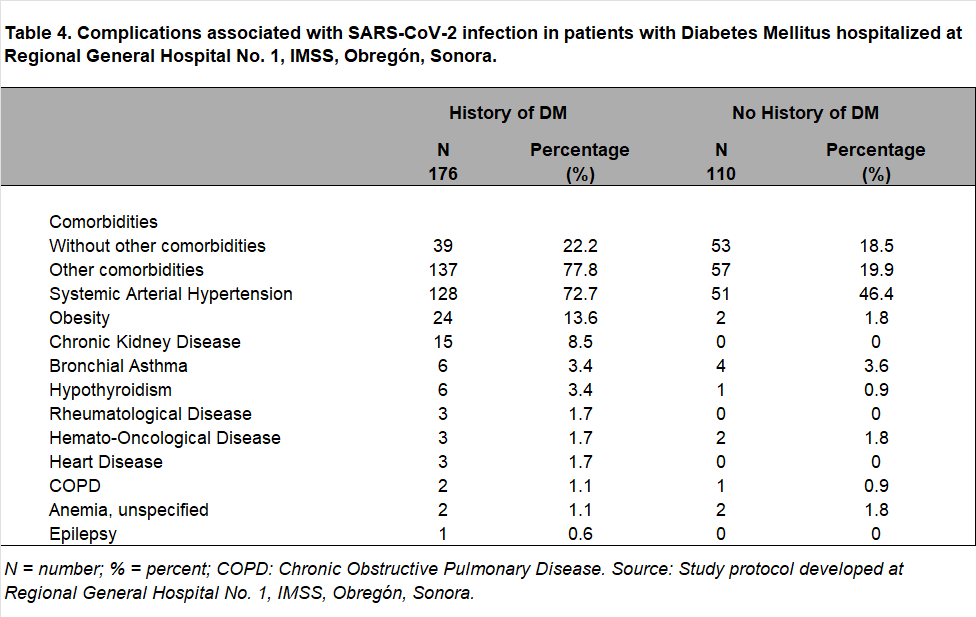
In the context of population health in Mexico and specifically in the state of Sonora, it is impossible to dismiss the role of other comorbidities. When obtaining the necessary data for the sample, it was impossible not to notice the existence of two or three comorbidities, so although they could have been taken as confounding agents, it was decided in this study to categorize them as effect modifiers and even analyzed the importance and effect of this variable on the appearance of complications in patients with DM hospitalized for COVID-19 in the hospital. Of the patients analyzed, in addition to having a history of Diabetes Mellitus, it was found that 77.8% presented other comorbidities, of which systemic arterial hypertension, obesity, and chronic kidney disease stand out. It was found that the coexistence of DM and another comorbidity has no relationship with complications, however, the coexistence of DM and two or more comorbidities does have a statistically significant relationship with the appearance of complications; according to Pinos-Robalino J.A.; The coexistence of comorbidities such as systemic arterial hypertension, heart disease, respiratory diseases, among others, can increase the risk of mortality. 29
Therefore, it is pertinent to mention that the objectives of this research work were met, finding relevant information consistent with the current literature concerning complications arising from SARS-CoV-2 infection in hospitalized patients with Diabetes Mellitus. As Hussain A. mentions in his research work, future research is necessary to promote progress in the understanding of the DM and COVID-19 binomial. 15
COVID-19 has become a disease of great global significance due to its ongoing pandemic. The implications and impact on the population, economy, and health services have been monumental. Therefore, research into all related factors has been of great importance and a source of work for the scientific community.
REFERENCES
1.Instituto Mexicano del Seguro Social. Diagnóstico y tratamiento farmacológico de la Diabetes Mellitus Tipo 2 en el primer nivel de atención [Publicado online]. 2018 [Revisado2020Nov4]. Disponible en: http://www.imss.gob.mx/sites/all/statics/guiasclinicas/718GER.pdf
2. Organización Mundial de la Salud. Informe mundial sobre la Diabetes [Publicado online]. 2016 [Revisado: 2020 Nov 4]. Disponible en: https://apps.who.int/iris/bitstream/handle/10665/254649/9789243565255spa.pdf;jsessionid=2E11B18CBCE287AC4812F3D1B3470A71?sequence=1
3. Machado-Villarroel L, Montano-Candia M, Dimakis-Ramírez DA. Diabetes Mellitus y su impacto en la etiopatogenia de la sepsis. Acta Médica Grupo Ángeles.2017;15(3):207–15.
4. Papatheodorou K, Banach M, Bekiari E, Rizzo M, Edmonds M. Complications of Diabetes 2017. J Diabetes Res. 2018;2018:1–4.
5.Torres-Tamayo M, Caracas-Portillo NA, Peña-Aparicio B, Juárez-Rojas JG, Medina-Urrutia AX, Martínez-Alvarado M del R. Infección por coronavirus en pacientes con diabetes. Arch Cardiol Mex [Publicado online]. 2020;90(91). Disponible en: http://dx.doi.org/10.24875/acm.m20000068
6. Bellido V, Pérez A. Consequences of COVID-19 on people with diabetes. Endocrinol Diabetes Nutr. 2020;67(6):355–6.
7. Li S, Wang J, Zhang B, Li X, Liu Y. Diabetes Mellitus and cause-specific mortality: A population-based study. Diabetes Metab J. 2019;43(3):319–41.
8. Wang K, Qiu Z, Liu J, Fan T, Liu C, Tian P, et al. Analysis of the clinical characteristics of 77 COVID-19 deaths. Sci Rep. 2020;10(1):16384.
9. López Pérez GT, Ramírez Sandoval M de LP, Torres Altamirano MS. Participantes de la respuesta inmunológica ante la infección por SARS-CoV-2. Alergia, Asma e Inmunología Pediátricas. 2020;29(1):5–15.
10. Guan W-J, Ni Z-Y, Hu Y, Liang W-H, Ou C-Q, He J-X, et al. Clinical characteristics of Coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708–20.
11. Suárez V, Suarez Quezada M, Oros Ruiz S, Ronquillo De Jesús E. Epidemiología de COVID-19 en México: del 27 de febrero al 30 de abril de 2020. Rev Clin Esp.12. Organización Mundial de la Salud. COVID-19 Weekly Epidemiological Update [Publicado online]. 2020 [Revisado: 2020 Nov 10]. Disponible en: https://www.who.int/publications/m/item/weekly-epidemiological-update---10 november-2020
13. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506.
14. Ouassou H, Kharchoufa L, Bouhrim M, Daoudi NE, Imtara H, Bencheikh N, et al. The pathogenesis of Coronavirus Disease 2019 (COVID-19): Evaluation and prevention. J Immunol Res. 2020;2020:1357983.
15. Hussain A, Bhowmik B, do Vale Moreira NC. COVID-19 and diabetes: Knowledge in progress. Diabetes Res Clin Pract. 2020;162(108142):108142.
16. Guo W, Li M, Dong Y, Zhou H, Zhang Z, Tian C, et al. Diabetes is a risk factor for the progression and prognosis of COVID-19. Diabetes Metab Res Rev. 2020;e3319.
17. Veronese N, Demurtas J, Yang L, Tonelli R, Barbagallo M, Lopalco P, et al. Use of corticosteroids in Coronavirus disease 2019 pneumonia: A systematic review of the literature. Front Med (Lausanne) [Publicado online]. 2020;7. Disponible en: http://dx.doi.org/10.3389/fmed.2020.00170
18. Huang I, Lim MA, Pranata R. Diabetes Mellitus is associated with increased mortality and severity of disease in COVID-19 pneumonia - A systematic review, meta-analysis, and meta-regression. Diabetes Metab Syndr. 2020;14(4):395–40
19. Yang JK, Feng Y, Yuan MY, Yuan SY, Fu HJ, Wu BY, et al. Plasma glucose levels and diabetes are independent predictors for mortality and morbidity in patients with SARS. Diabet Med. 2006;23(6):623–8.
20. Zhu L, She Z-G, Cheng X, Qin J-J, Zhang X-J, Cai J, et al. Association of blood glucose control and outcomes in patients with COVID-19 and pre-existing type 2 diabetes. Cell Metab. 2020;31(6):1068-1077.e3.
21. Yang J, Zheng Y, Gou X, Pu K, Chen Z, Guo Q, et al. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: a systematic review and meta-analysis. Int J Infect Dis. 2020;94:91–5.
22. Basto-Abreu A, Barrientos-Gutiérrez T, Rojas-Martínez R, Aguilar-Salinas CA, López-Olmedo N, De la Cruz-Góngora V, et al. Prevalencia de diabetes y descontrol glucémico en México: resultados de la Ensanut 2016. Salud Publica Mex. 2020;62(1):50–9.
23. Mauricio Hernandez Avila Juan Rivera Domarco Teresa Shamah Levy Lucia Cuevas Nasu et al. Encuesta Nacional de Salud y Nutrición de Medio Camino 2016 (ENSANUT 2016) Informe final de resultados [Publicado online]. 2016. Disponible en: https://www.gob.mx/cms/uploads/attachment/file/209093/ENSANUT.pdf
24. Rojas-Martínez R, Basto-Abreu A, Aguilar-Salinas CA, Zárate-Rojas E, Villalpando S, Barrientos-Gutiérrez T. Prevalencia de diabetes por diagnóstico médico previo en México. Salud Publica Mex. 2018;60(3):224–32.
25. Gobierno de México, Centro de Investigación en Allimentación y Desarrollo. Sonora dentro de las entidades con mayor sobrepeso y obesidad a nivel nacional [Publicado online]. Centro de Investigación en Alimentación y Desarrollo. 2020 [Revisado 2020 Dic 20]. Disponible en: https://www.ciad.mx/notas/item/2397sonora-dentro-de-las-entidades-con-mayor-sobrepeso-y-obesidad-a-nivel-nacional
26. Instituto Mexicano del Seguro Social. Informe al Ejecutivo Federal y al Congreso de la Unión sobre la situación financiera y los riesgos del Instituto Mexicano del Seguro Social 2017-2018 [Publicado online]. 2018 [Revisado: 2020 Nov 4]. Disponiblehttp://www.imss.gob.mx/sites/all/statics/pdf/informes/20172018/21InformeCompleto.pdf
27. Secretaría de Salud de Sonora. Situación de la infección respiratoria aguda por SARS-CoV-2, COVID-19: Nota técnica 22:30 horas. Diciembre 14 de 2020 [Publicado online]. 2020 [Revisado 2020 Dic 17]. Disponible en: http://covid19.saludsonora.gob.mx/wp-content/uploads/2020/12/AVISO EPIDEMIOLOGICO-COVID19-Dic.14.2020.pdf
28. Instituto Mexicano del Seguro Social. Base SINOLAVE de Hospital General Regional No. 1 Ciudad Obregón, Sonora. SINOLAVE. 2020.
29. Pinos Robalino PJ, Segovia Palma P, Cedeño Delgado MJ, Gonzabay Bravo EM. La diabetes y las complicaciones con el covid-19. RECIMUNDO. 2020;4(4):509–16.
Citation
Castillo-Chapa JA and Ruiz-Valdez CA, Complications associated with SARS-Cov-2 infection in hospitalized patients with diabetes mellitus, ERSJ 2026,1(3) 99-110
Academic Editor: David Alejandro Cabrera Gaytan, Received: 13 April 2025, Revised: 20 May 2025, Accepted: 28 May 2025, Published: 18 January 2026.