Epidemiological surveillance of cholera in the 21st century
by Oscar Cruz-Orozco*
*Coordinación de Vigilancia Epidemiológica Instituto Mexicano del Seguro Social, Ciudad de México 03100, México.
More than a century and a half has passed since John Snow's observations on the spread of cholera in London. Even though the causative agent was unknown, the hypothesis of waterborne and foodborne transmission proved correct.
In 1854, the causative agent of the disease, Vibrio cholerae, had been identified by Filippo Pacini; however, credit for the discovery was given to Robert Koch 30 years later.
Vibrio cholerae is a Gram-negative, facultative anaerobic bacillus, classified into 198 serotypes based on the somatic antigen "O." Serotype O1 is pathogenic, although serotype O139 has also been identified in India. Therefore, this characteristic is commonly referred to as O1 and Non-O1, which includes O139.
Serotype O1 is divided into biotypes: Classical and Tor. They are further divided into three serotypes: Inaba, Ogawa, and Hikojima. Cholera toxin is the primary virulence factor of Vibrio cholerae O1.
Living conditions in developed countries have virtually eliminated cholera. The cases that do occur are imported from countries where the disease remains endemic.
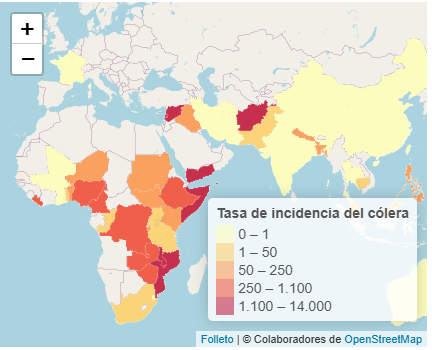
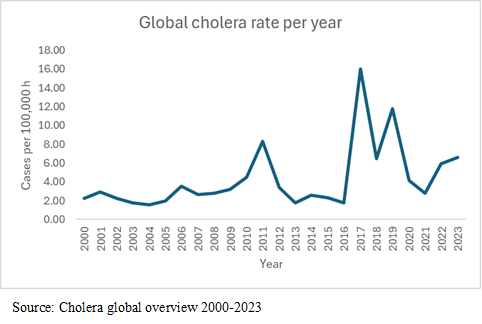
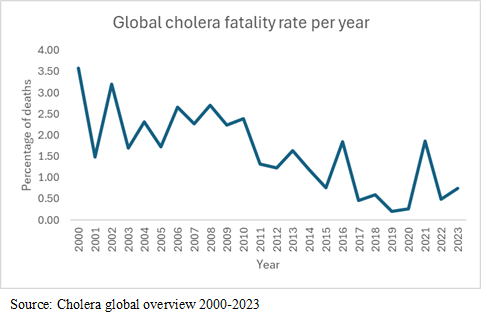
Since 2000, a periodic increase in cases has been observed, especially in the Middle East and Africa. 2017 saw the highest number of cases this century, with 1,227,392 cases reported, with the most cases occurring in Yemen, Haiti, the Dominican Republic, and Somalia. Despite the upward trend, a decrease in case fatality has been observed worldwide.
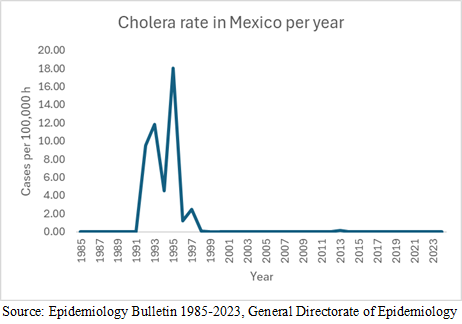
In Mexico, one case was reported in 2018, and there have been no subsequent cholera cases, despite the high migration of Haitians to the north of the country. Official records indicate an outbreak in 2013 with its epicenter in the state of Hidalgo, reaching 187 patients diagnosed with cholera due to toxigenic Vibrio cholerae O:1 Ogawa; in 2014, 15 cases were confirmed, 14 of which were serotype O1 Ogawa and one of which was serotype O1 Inaba toxigenic; in 2015, one case of toxigenic Ogawa was confirmed, and in 2016, one case of toxigenic Ogawa was confirmed. Previously, in the mid-1990s, there was an explosive increase in cases, with the highest number of cases occurring in 1995, reaching 16,430 cases and a fatality rate of 1.1%. The most affected states were Yucatán, Campeche and Chiapas.
In 2024, Yemen was the country with the most reported cholera cases, with 260,552, followed by Afghanistan with 175,262 cases, and Pakistan with 77,217. Togo, located on the African continent, had the highest case fatality rate, with 6.03%.
In 2025, as of July 21, 355,848 cases of cholera had been reported worldwide, with the countries with the most cases being Afghanistan (89,882), South Sudan (68,206), and Yemen (50,015).
You can consult:
1.Secretaría de Salud, Manual de Procedimientos Estandarizados para la Vigilancia Epidemiológica de la Enfermedad Diarreica Aguda (EDA), México, 2022.
2.Secretaría de Salud, Manual de Procedimientos Estandarizados para la Vigilancia Epidemiológica de Cólera, México, 2012.
3.Secretaría de Salud, Programa Nacional de Prevención y Control del Cólera 2001 Manual para la Vigilancia epidemiológica del Cólera en México, México, 2021.
4.DGE, Boletín epidemiológico, Sistema Nacional de Vigilancia Epidemiológica, Sistema Único de Información. Vol 1, Num 1 1985 a 2023.
5.WHO, Cholera global overview 2000-2023,
Citation
Cruz-Orozco O Epidemiological surveillance of cholera in the 21st century, ERSJ2025,1(1) 41-44