Antiretroviral therapy adherence in patients with HIV/AIDS and family functionality
Leonardo Fabián-Yáñez Gutiérrez and Miguel Ángel Aguilera-Arias
Instituto Mexicano del Seguro Social,Hospital General de Zona No. 5, México 15D, 84094, Heroica Nogales, Sonora.
Abstract
Introduction: Adherence to antiretroviral treatment in patients with HIV/AIDS worldwide has a prevalence of 55%. Poor adherence to treatment is a risk factor for complications such as AIDS, genetic resistance to the drug, and multiple hospital admissions, impacting the patient's quality of life. Risk factors for poor treatment adherence have been found to include lack of patient awareness, lack of family and/or social support, and substance abuse.Objetive: To describe the perception of family functionality and antiretroviral therapeutic adherence in patients with HIV/AIDS.
Materials and methods: An analytical, retrospective, cross-sectional, prevalence study was conducted. 125 patients participated, obtaining a proportional sample. A univariate analysis of the qualitative variables was performed, cross-tabs with independent variables and dependent variable. The quantitative variables were measured by measures of dispersion and central tendency. The instruments used were the family APGAR questionnaire and SMAQ
Results: It was obtained that the independent variable (“Family functionality”) and the dependent variable (“Treatment adherence”), 50 responses are “Adherent” representing 40% and 75 responses are “Non-adherent” representing 60%. The “Family functionality” based on the classification was obtained “Normal functionality” with 114 cases (91.2%), “Mild dysfunctionality” with 2 cases (1.6%), “Moderate dysfunctionality” with 4 cases (3.2%) and “Severe dysfunctionality” with 5 cases (4%).
Conclusions: Treatment adherence was not significantly associated with family functioning.
Keywords: Treatment adherence, family functionality, Acquired Immunodeficiency Syndrome, Human Immunodeficiency Virus.
INTRODUCTION
Adherence to antiretroviral therapy can be understood as: a patient's ability to be involved in the selection, initiation and monitoring of antiretroviral therapy (ART), leading to rigorous compliance with the main objective of achieving suppression of viral replication. There are a large number of variables that impact adherence to antiretroviral therapy in patients diagnosed with HIV (Human Immunodeficiency Virus) / AIDS (Acquired Immune Deficiency Syndrome), which include: those related to medication, socioeconomic factors, psychological and sociodemographic factors, level of knowledge of the disease and the treatment itself1. Adherence to HIV/AIDS treatment is of critical importance as a decisive factor in a person's life. This is due to the rapid replication and mutation of the virus, which requires good pharmacological adherence to achieve lasting viral suppression 2. Furthermore, non-adherence is a risk factor that increases the likelihood of complications such as AIDS, genetic drug resistance, and multiple hospital admissions, impacting the patient's quality of life 3.
Among psychological factors, interpersonal issues may involve the family, which plays a role of family support and perceived social and familial esteem 4. The family is considered an institution and/or group of individuals, whether blood-related or not, who live under the same roof; or it is perceived as the union of people who share a long-term life project, in which feelings of permanence are generated, thereby developing a personal commitment among its members and establishing relationships of intimacy, reciprocity, and dependence 5. The family plays a fundamental role in the management of chronic pathologies, as they activate self-regulation mechanisms, thus achieving homeostasis within their functionality and causing changes in family interactions. These changes in interactions, whether conscious or unconscious, can generate complex situations of balance or imbalance, jeopardizing family well-being and patient management 6. Worldwide, the prevalence of people living with HIV in 2020 was 37.7 million; the incidence for the same year was 1.5 million, and 680,000 people died from an AIDS-related illness 7.
The prevalence of HIV in Mexico from 1983 to the fourth quarter of 2021 is a total of 331,437 reported cases. The prevalence rate in men was 270,035 cases (81.5%) and in women 61,402 (18.5%).
In Lima, Peru, a study was conducted among patients with HIV/AIDS, which revealed normal family functioning (43%), mild dysfunction (23%), severe dysfunction (21%), and moderate dysfunction (13%) 8.
At Family Medicine Unit No. 53 in León, Guanajuato, Mexico, in 2020, the Family APGAR instrument was administered to a sample of 71 participants, with a single selection criterion of HIV/AIDS. Results were obtained of good family functioning (36%), mild family dysfunction (27%), severe family dysfunction (27%), and moderate family dysfunction (10%) 9.
A meta-analysis conducted in 2010 with a total of 23 observational studies compiled, with a total of 9,931 participants over 18 years of age and receiving HAART, concluded that 55% of patients had treatment adherence greater than 90% 10.
At General Hospital of Zone No. 15, Dr. José Zertuche Ibarra, Mexican Social Security Institute, in Reynosa, Tamaulipas, obtained the results of adherence to antiretroviral treatment. 90.3% responded that in the last week they had taken the drugs based on medical indications; only 9.7% did not take the medication as prescribed 11.
In 2018, a study was conducted in Centro Habana, obtaining a statistical association in the family functioning variable with a p < 0.05 and an odds ratio = 6. Concluding that family dysfunction was a risk factor for poor therapeutic adherence to HAART (Highly Active Antiretroviral Therapy) 12. Another study conducted in 2002, which used an observational, prospective (9-month) methodology at the Son Duretal Hospital, located in the Balearic Islands, Spain; In a study involving a total of 202 participants, the variable of living status (independent or with a partner and parents or family) was not statistically significant as a factor in non-adherence to antiretroviral drugs.
Therefore, the objective of this study was to describe the perception of family functioning and antiretroviral therapy adherence in patients with HIV/AIDS.
MATERIALS AND METHODS
A descriptive, cross-sectional study was conducted during the months of August and September 2023 at General Hospital Zone No. 5 in Nogales, Sonora.
The selection criteria for participation in the survey were: patients over 18 years of age with HIV/AIDS, who agreed to participate in the study by signing an informed consent form, and who were receiving treatment with an antiretroviral drug.
Patients with psychiatric conditions, those undergoing a study protocol for HIV/AIDS confirmation, those who did not agree to participate in the protocol, and those recently diagnosed with HIV/AIDS (less than 4 months ago) were excluded.
Surveys without complete responses were eliminated (surveys with a minimum of 80% completed).
Using the nominal census of current patients diagnosed with HIV/AIDS who attended follow-up visits from 1998 to 2021, a total of 139 patients were identified, ranging in age from 20 to 83 years. The sample size calculation formula for a proportion of a finite universe was used, yielding a sample size of 123.
The dependent variable was adherence to antiretroviral therapy, while the independent variables were family functioning, defined as a family's ability to maintain balance in a changing environment. Sex, age, duration of antiretroviral therapy, marital status, and educational level were also taken into account.
To assess therapeutic adherence, the Simplified Medication Adherence Questionnaire (SMAQ), validated in 1998-1999 in the Spanish community, was used. To identify participants' perceptions of family functioning, the Family APGAR survey was administered. Sociodemographic variables were added to the survey to describe the study population.
The research did not pose any risks to participants, as data was collected through physician-patient surveys. Furthermore, the study protocol was submitted to the local research committee and approved for implementation.
A univariate analysis was performed, describing the quantitative variables through measures of central tendency and dispersion. The bivariate analysis used the chi-square test for categorical variables. The statistical software programs Excel and SPSS® version 25.0 for Windows® were used.
RESULTS
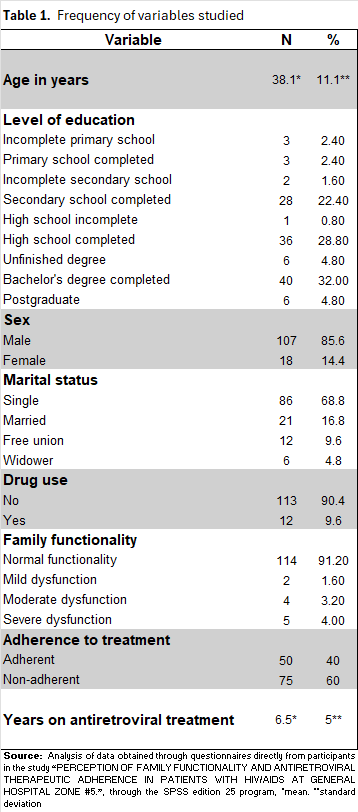
A sample of 125 participants surveyed was analyzed. The average age of the population was 38.1 years. Regarding education, the highest percentage had a bachelor's degree (32%). The majority were male, with 85.6% (107), and 90% (113) denied using any type of drug. The predominant marital status was single, with 68% (86).
The variable "Family Functionality" was categorized as: "Normal Functionality," "Mild Dysfunction," "Moderate Dysfunction," and "Severe Dysfunction." The frequencies obtained were "Normal Functionality" with 114 cases (91.2%), "Mild Dysfunction" with 2 cases (1.6%), "Moderate Dysfunction" with 4 cases (3.2%), and "Severe Dysfunction" with 5 cases (4%). The frequencies obtained are presented in Table 5. The frequency of the dependent variable "Treatment Adherence" was 40% (50). The average duration of antiretroviral treatment was 6.5 years. Table 1
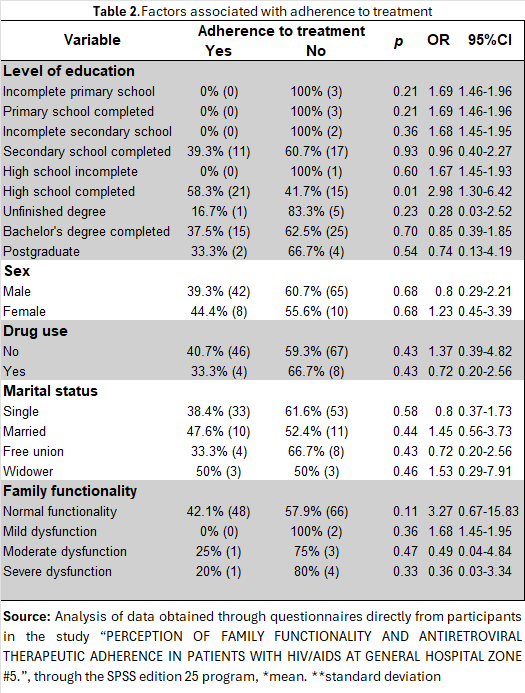
The result that presented statistical significance was "High School Completion," with p = 0.008. A relationship was found between the two variables: OR = 2.98 and 95% CI = 1.30-6.42. The remaining categories within each variable were not statistically significant. Table 2.
DISCUSSION
The results obtained for the independent and dependent variables were compared with those reported in the theoretical framework. The order in which the data were contrasted followed both international and national levels. It is worth noting that the literature reviewed did not include state-level information for either variable; therefore, data from another state within the country were used as a national reference.
Lizano Pastrano (2019), in Lima, Peru, reported perceptions of normal family functionality in 43% of participants, mild dysfunction in 23%, severe dysfunction in 21%, and moderate dysfunction in 13% [8]. In comparison, the present study showed 91.2% normal family functionality, 1.6% mild dysfunction, 3.2% moderate dysfunction, and 4% severe dysfunction.
Caldera Guzmán et al. (2020), in Guanajuato, Mexico, found 36% of participants perceived normal family functionality, 27% mild dysfunction, 10% moderate dysfunction, and 27% severe dysfunction [9]. Compared with the results of the present study—91.2% normal family functionality, 1.6% mild dysfunction, 3.2% moderate dysfunction, and 4% severe dysfunction—our findings indicate higher perceptions of normal family function and lower levels of dysfunction across all categories. Ortego et al. (2011), conducted in Spain, showed that 55% of patients achieved treatment adherence greater than 90% [10]. In the present protocol, adherence to antiretroviral therapy was 40%, while non-adherence reached 60%.
Hernández et al. (2012), conducted in Reynosa, Tamaulipas, reported that 90.3% of participants adhered to antiretroviral treatment over the past week according to medical indications, while only 9.7% did not take their medication as prescribed [11]. Compared to these findings, our study demonstrates a lower level of adherence to antiretroviral therapy.
It is concluded that the population studied in this research protocol provided a general overview of the status of the evaluated variables at the time. The results indicate that adherence to antiretroviral therapy in this population is lower when compared with both national and international studies. Regarding family functionality, the proportion of participants reporting normal family function was higher, while all categories of dysfunction (mild, moderate, and severe) were lower compared to other studies at both national and international levels.
The recommendations derived from this study include exercising particular caution with the subgroup of individuals who have completed high school, in order to improve adherence to antiretroviral therapy. Multidisciplinary support is also advised to identify underlying causes of non-adherence and to develop targeted interventions.
Finally, no association was found between family functioning and adherence to antiretroviral treatment.
REFERENCES
1.Betancourt-Gambino J. Adherencia al tratamiento antirretroviral en pacientes seropositivos. Rev Cubana Med Gen Integr [Internet]. 2018 [citado 31 de marzo de 2022];34(3). Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S086421252018000300010
2.Vilató-Frómeta 2.- L, Martín-Alfonso L, Pérez-Nariño I. Adherencia terapéutica y apoyo social percibido en personas que viven con VIH/sida. Rev Cubana Salud Pública [Internet]. 2015 [citado 2 de abril de 2022];41(4):620–30. Disponible en: https://www.redalyc.org/ articulo.oa?id=21443545005
3.Hernandez-Gomez A., Rodriguez-Rios T., Duran-Badillo T., Vázquez-Galindo L., Gutiérrez-Sanchez G., Garcia-Castillo G. Adherencia al tratamiento antirretroviral en pacientes con VIH/SIDA. Rev Enferm Inst Mex Seguro Soc [En línea]. 2013 [Consultado el 18 de abril de 2022]; 21 (2): [85-90] Disponible en: file:///E:/Adherencia%20al%20tratamiento%20en%20pacientes%20con%20VIH.pdf
4.Sánchez-Peña S, Pastor-Bravo MM, Cánovas-Tomás MA, Almansa-Martínez P, Peñalver-Guillén C, Jiménez-Ruiz I. Factores relacionados con la adherencia al tratamiento antirretroviral en mujeres con VIH: un estudio mixto con diseño secuencial. Enferm Glob [Internet]. 2021 [citado 31 de marzo de 2022];20(62). Disponible en: https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1695-61412021000200001
5.Fernández-Ortega M. El impacto de la enfermedad en la familia. Rev Fac Med UNAM [Internet]. 2004 [citado 2 de abril de 2022];47(6):251–4. Disponible en: https://www.medigraphic.com/pdfs/facmed/un-2004/un046f.pdf
6.ONUSIDA. Últimas estadísticas sobre el estado de la epidemia de sida [Internet]. Ginebra: Organización Mundial de la Salud; 2021 [citado 2 de abril de 2022]. Disponible en: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_es.pdf
7.Lizano-Pastrano KY. Funcionalidad familiar en pacientes con VIH/SIDA del Hospital de Ventanilla [Tesis en Internet]. Lima: Universidad César Vallejo; 2019 [citado 24 de abril de 2022]. Disponible en: https://repositorio.ucv.edu.pe/handle/20.500.12692/48809
8.Caldera-Guzmán D, Pacheco-Zavala MP. Funcionalidad familiar del paciente con VIH/SIDA en una Unidad de Medicina Familiar de León, Guanajuato. El Residente [Internet]. 2020 [citado 24 de abril de 2022];15(2):48–53. Disponible en: https://www.medigraphic.com/pdfs/residente/rr-2020/rr202b.pdf/
9.Ortego C, Huedo-Medina TB, Vejo J, Llorca J. Adherence to highly active antiretroviral therapy in Spain: a meta-analysis. Gac Sanit [Internet]. 2011 [citado 15 de octubre de 2022];25(4):282–9. Disponible en: https://www.gacetasanitaria.org/es-adherence-highly-active-antiretroviral-therapy-articulo-S0213911111000501
10.Hernández-Gómez A, Rodríguez-Ríos T, Durán-Badillo T, et al. Adherencia al tratamiento antirretroviral en pacientes con VIH/SIDA [Tesis en Internet]. Tamaulipas: Universidad Autónoma de Tamaulipas, Unidad Académica Multidisciplinaria Matamoros; 2012 [citado 15 de noviembre de 2023]. Disponible en: https://www.medigraphic.com/ pdfs/enfermeriaimss/eim-2013/eim132e.pdf
11.Bastán J, Vian-Castaño L. Factores asociados a la no adherencia terapéutica a los antirretrovirales en personas con VIH/sida. Rev Cubana Med Trop [Internet]. 2020 [citado 15 de octubre de 2022];72(2). Disponible en: http://scielo.sld.cu/scielo.php? script=sci_arttext&pid=S0375-07602020000200003
Citation
Fabián-Yáñez L and Aguilar-Arias MA, Antiretroviral therapy adherence in patients with HIV/AIDS and family functionality, ERSJ 2025,1(1)27-34
Academic Editor: Mónica Rivera Mahey, Received: 13 April 2025, Revised: 10 May 2025, Accepted: 16 May 2025, Published: 16 May 2025.