Postpartum depression is associated with the route of obtaining the newborn
Briana Bray-Contreras and Eduardo Arturo Serrano-García
Hospital General de Zona No. 14, Instituto Mexicano del Seguro Social, C. República de Cuba, El Mirasoles, 83120 Hermosillo, Sonora.
Abstract
Introduction: Postpartum depression is a condition where the disorder arises during the puerperium as a response to biochemical, hormonal, psychological, and social changes. It has an incidence of 10 to 15% and is the most common psychiatric disorder in the puerperium. It may be related to the mode of delivery and is often indirectly associated with sociodemographic factors.Objetive: To determine whether postpartum depression is associated with the route of obtaining the newborn.
Materials and methods: A prospective, observational, and descriptive epidemiological study was conducted with 189 patients with 24–48 hours of postpartum period. They were selected by simple random sampling based on consecutive cases using the 10-item Edinburgh Postnatal Depression Scale (EPDS). Results were interpreted using descriptive statistics with incidence and χ2 for dichotomous variables using SPSS, as well as relative risk for postpartum depression depending on the route of obtaining the newborn.
Results: The overall incidence of postpartum depression in the study population was 18.28%. The χ2 statistic was 74.86, with a p-value of <0.001, indicating that the mode of delivery is significantly associated with the development of postpartum depression (p <0.05). Women who received cesarean delivery were 2.09 times more likely to develop postpartum depression (DPP) compared to women who received vaginal delivery.
Conclusions: The study demonstrated that cesarean delivery was significantly associated with DPP.
Keywords: Puerperium, postpartum depression, route of obtaining the newborn.
INTRODUCTION
Pregnancy is a complex biopsychosocial experience, with childbirth being a crucial moment. This is defined as the exit of one or more fetuses from the interior of the uterine cavity to the exterior. It begins with the first perceptible uterine contractions and ends with delivery. 1
This event can occur vaginally, where the bony pelvis constitutes the canal through which the fetus must pass. Through this route, various cervical modifications occur, such as enlargement of the lower segment, effacement and dilation of the cervix (passive production as the fetus propels through the cervix), expulsion of the mucous plug, and engagement. This is where the fetus begins to descend and successfully cross the birth canal. 2
It is important to understand the processes a woman goes through from the beginning of her pregnancy, explain their definition, and the types of birth canals through which the birth of the child may be possible. Define what depression is and, in more detail, what postpartum depression means, its phases, international, national, and local incidences, as well as the risk factors that may influence its onset.
Prospective studies have shown that mood and anxiety symptoms increase in the puerperal state, as does the risk of depression after childbirth. Therefore, once they are identified, the first step is an assessment to determine their severity. 3
The Diagnostic and Statistical Manual of Mental Disorders, in its fifth edition (DSM-V), included major depressive disorder with onset in the peripartum period or in the first four weeks postpartum. 4 This indicates that, for diagnosis, five or more of the following symptoms must be present for at least two weeks: depressed mood, lack of interest or pleasure in activities, sleep disturbance, loss/lack of energy, psychomotor agitation or retardation, excessive feelings of guilt, decreased concentration, or suicidal thoughts. There is little evidence regarding the mode of delivery, considering variables such as parity, income, marital status, and area of residence. Therefore, it is helpful to understand a little more about the patient's context and discuss whether these have any impact on her emotional state.
It has been described that one of the relevant factors that affect the mother's perception and, therefore, her choice of mode of delivery is the experiences of the pregnant mother and the associated pain. This can generate psychological effects on her that can even increase the likelihood of suffering from PPD. That said, it is important to generate evidence that allows us to understand the factors that influence the development of this condition, including perceptions of the mode of delivery 2, as well as factors such as parity, socioeconomic status, and type of housing.
The postpartum period is a period of great biopsychosocial vulnerability for the mother due to the multiple changes it entails. The emotions experienced increase exponentially, whether due to insecurity in caring for the newborn, postpartum discomfort, excessive visits, and the discrepancy between the information the mother receives from professionals and those close to her. 5
Globally, 70% of depressions present with physical symptoms, especially pain. Doctors associate these complaints with other illnesses and refer the mother to other professionals rather than a psychologist or psychiatrist, which can lead to a sustained increase in morbidity, a significant increase in the risk of developing other illnesses, and a decrease in quality of life. 6
In Mexico, as in other countries, depression is found more in women than in men, with a difference of 10.4% and 5.4%, respectively. According to a meta-analysis, the prevalence of postpartum depression is estimated at 12%. There are also nine studies on the prevalence of this condition, ranging from 6.6% to 24.6% based on clinical interviews in urban areas. In the rural population, only two studies have been published, which estimate prevalences between 11% and 12.9%. 7
Finally, the objective of the study is to determine whether postpartum depression is associated with the mode of delivery.
MATERIALS AND METHODS
A prospective, observational, and descriptive study was conducted to investigate the presence of postpartum depression (DPP) among women in the gynecology and obstetrics department located on the first floor of the General Hospital of Zone No. 14 with a Burn Unit (HGZ 14).
Women in the immediate postpartum period in the gynecological inpatient unit who had delivered vaginally or by cesarean section with a live fetus, assigned to General Hospital of Zone No. 14, were included.
Puerperal women with a previous diagnosis of depression or a history of taking antidepressant medication at the time of the survey, as well as those who had died, were excluded.
Patients with mental impairment, physical or visual limitations that prevented them from completing the interview and completing the questionnaire, or those who were unable to read or write, were also excluded. The surveys were incomplete or unreadable, impeding the interpretation of each of the variables of interest, as well as those who dropped out of the study before completing the project.
The population consisted of 2,258 pregnant patients who completed their pregnancies either vaginally or by abdominal delivery in 2022 at the General Hospital of Zone No. 14 8. The finite population formula was used to calculate the sample, with a 95% CI and a statistical significance of ≤0.05, of which 186 were determined.
The dependent variable was postpartum depression, and the independent variables were: method of obtaining the product, occupation, housing, income, marital status, and parity.
The instrument used was the Edinburgh Postpartum Depression Scale (EPDS), a screening tool developed from the Irritability, Depression, and Anxiety Scale. This instrument has advantages that facilitate the discussion of emotional problems and the monitoring of the clinical course of postpartum depression. It is one of the most widely used scales for postpartum depression and has been validated in national studies. 9, 10, 11, 12
Each patient in the gynecology inpatient unit who met the study entry criteria was asked to participate in the study, and informed consent was obtained. The study was submitted to the local research committee and approved.
During the research period, the privacy of the research subject was confidentially protected, respecting the individual's bioethical principles of beneficence, nonmaleficence, autonomy, and justice.
Descriptive statistics were used to interpret the results through measures of central tendency (mean, frequencies, and percentages). Incidence was initially calculated as percentages, and a comparison was then made by delivery mode (vaginal or cesarean) to support or refute the working hypothesis with the results as a total percentage. Statistical analysis was performed to compare dichotomous variables using 2 and the analysis was carried out using the Statistical Package for the Social Sciences version 29 (SPSS v.29) statistical data package.
RESULTS
This study included 186 postpartum patients treated at the Burn Unit of Zone No. 14 General Hospital. Of the total patients (n=186), the mean age was 26.44 years (SD 5.67), indicating moderate variability in age distribution. The majority lived in urban dwellings, representing 95.16% of the sample, while only a small percentage, 4.84%, came from rural areas (Table 1).
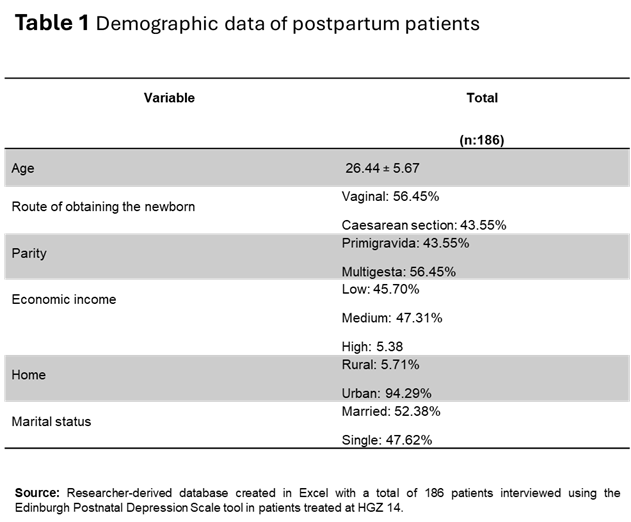
Regarding socioeconomic and personal characteristics, the reported occupations showed that 45.16% of the patients were homemakers and 40.32% were wage earners, reflecting the occupational diversity of the study participants.
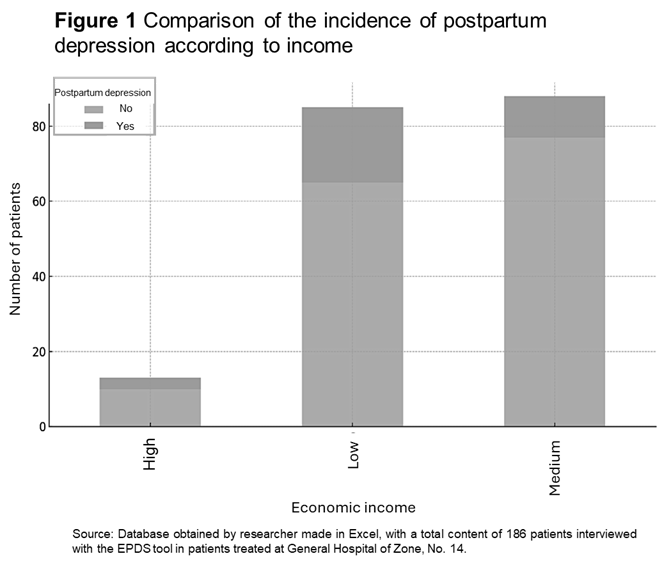
The marital status of the patients was as follows: 51.61% were civilly married and 48.39% were single. In terms of income, almost half of the sample (47.31%) reported incomes between $6,000 and $10,000 or less than $5,000, which could indicate a predominant middle-to-low socioeconomic status in the sample. (Figure 1).
Using the EPDS, any patient who obtained a score ≥ 13 points was considered positive for DPP. According to the above, the overall incidence of postpartum depression in the study population was 18.28%, which is a high percentage compared to the reviewed history of DPP in Sonora.
The group of women who delivered vaginally had an incidence of 12.38%, while the incidence of women who delivered via cesarean section was 25.93%.
The risk ratio (RR) showed that women who had a cesarean section had a 2.09-fold higher risk of developing postpartum depression compared to those who had a vaginal delivery.
The chi-square statistic was 74.86, with a p-value of <0.001, indicating that the mode of delivery was significantly associated with the onset of postpartum depression (p <0.05). Specifically, patients who underwent a cesarean section had a higher incidence of postpartum depression compared to those who had a vaginal delivery.
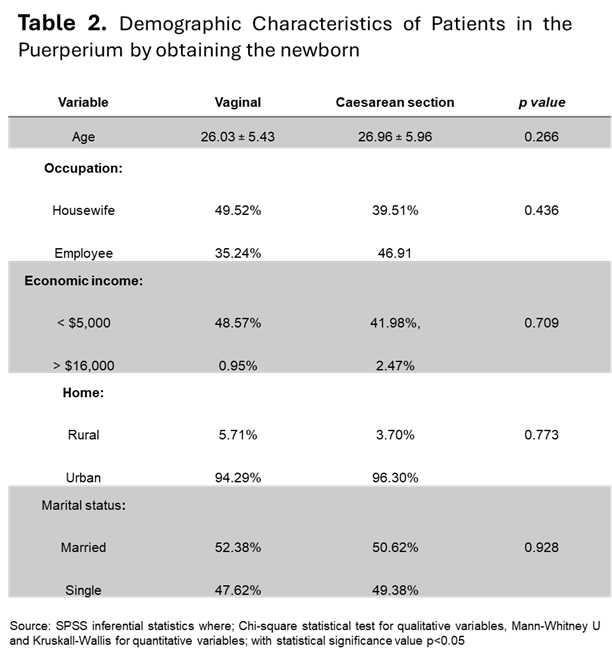
The results of the demographic table indicate no statistically significant differences between the groups of women who had a vaginal delivery and those who had a cesarean section in terms of age, occupation, income, housing type, and marital status. The statistical tests applied (chi-square, Mann-Whitney U, and Kruskal-Wallis) confirmed the demographic homogeneity between the two groups. (p > 0.05) (Table 2).
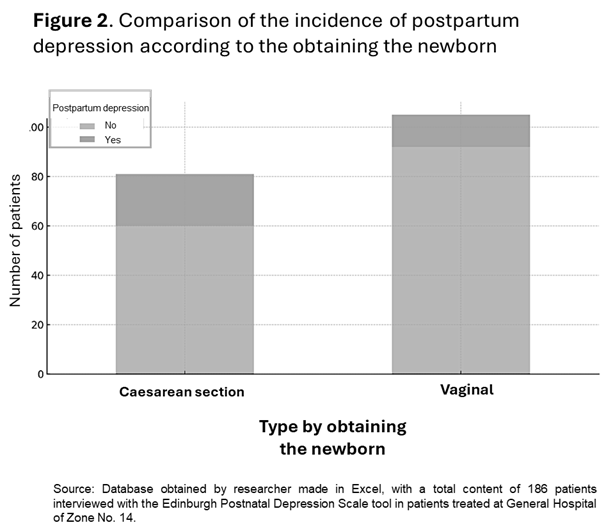
Regarding DPP and number of pregnancies, a total of 19 multipregnant women with a positive DPP test were found, 9 of them with vaginal delivery and 10 with cesarean delivery. Sixteen primigravidae women with DPP were found using the EPDS tool, 4 of them with vaginal delivery and 11 with cesarean delivery. This indicated that multipregnant patients had a higher frequency of DPP. (Figure 2)
DISCUSSION
The overall incidence of DPP was 18.28%. This indicates that we are slightly above the percentages of postpartum depression indicated by the World Health Organization, which are 10 to 15% or what has been reported in the state of Sonora.13 However, it is lower than what has been reported in other studies, which can reach 50.7%. 14
When analyzing the type of delivery, it was observed that the incidence of DPP in the group of women who had cesarean sections was 25.93%. This percentage was provided by 21 patients with a positive EPDS test, which confirmed the working hypothesis due to the high incidence in that group.
The chi-square result was 74.86, with a p-value of <0.001, indicating that cesarean delivery is significantly associated with the development of DPP (p <0.05). This has not been studied in depth in a prospective analysis in women without a history of depression, which is why screening and closer observation of these patients during their hospital stay is advisable.
In the group of women who delivered vaginally, the incidence of DPP was 12.38%, which is very similar to the international, national, and local average.
Women who delivered their baby by cesarean section, due to undergoing a major surgical procedure, had a longer hospital stay of 48 hours due to observation by the attending physician, greater pain during recovery, and a documented lower concentration of oxytocin, adrenaline, and noradrenaline, which slows maternal recovery and the onset of mother-child bonding.
Because the Mexican Social Security Institute (IMSS) varies widely in coverage, it was found that 95.2% of patients come from urban areas (Hermosillo, Sonora), which indicates that these patients have fewer social limitations compared to those without health insurance.
The women studied, based on their socioeconomic and personal factors, show a high percentage of employment as homemakers, which implies greater time with the newborn.
Regarding monthly income, 47% are from a lower-middle socioeconomic level, with a monthly salary between less than five thousand and ten thousand pesos. Fifty-six percent of the women studied are pregnant with multiple children, which can create fear in the future about the new challenge with their other children. Financially, being a homemaker dependent on her partner to purchase hygiene items for the newborn, clothing, and, above all, not neglecting the needs of the rest of the family, affects the economy. On the other hand, a higher percentage of patients with DPP was found in multipregnancies, which corresponds to the literature consulted according to Clinical Practice Guide 15. Due to this research, a considerable incidence of suspected postpartum depression in postpartum women within the first 24 to 48 hours was determined, exceeding the international average of 10 to 15%.
Many of these patients tested positive for the EPDS tool. They reported constant crying, not always for a specific reason, fear about the future and how they carried out their daily lives with a new member of their family; feeling constantly nervous or restless, with difficulty sleeping, which can be detrimental to the mother, the child, and the family environment. There is evidence that anemic states due to a progressively shorter sleep routine of less than 6 hours can be detrimental in the long term, as the body cannot rest fully, and waking up can be irritating to start the new day.
These types of events had not been documented in the northwest of the country, as there were no previous studies comparing the variable of delivery route with the onset of postpartum depression. This is useful for recognizing patients who need to pay closer attention when monitoring their postpartum status. This research will serve as a guideline for initiating new studies in the region, as well as for follow-up care, since, according to the literature, this condition may occur more frequently two to three months after delivery. This opens the possibility of studying a larger number of patients to obtain a more complete population.
It is worth mentioning that a higher level of postpartum depression could have been found if a longer follow-up period had been conducted, with patients in the puerperium approximately two months after the birth of their baby.
Being a prospective study, there are several limitations, especially within the hospital, since we do not receive a high influx of patients in the inpatient area because the majority of the population for vaginal and cesarean births is treated at the Pediatric Gynecology Hospital. A similarly prospective study is recommended, but with the involvement of the psychiatric and psychological staff at the unit, to provide comprehensive care to the patient suspected of having postpartum depression and to manage her postpartum period in a much more personally enjoyable way, with the mother-child bond.
REFERENCES
1. Carvajal-Jorge, Barriga-Mária (2020). Manual de obstetricia y ginecología. 11.a Versión On-Line. Chile: Pontificia Universidad Católica de Chile. [Internet] [Update 2020, Consulted el 18 de Junlio de 2023]
2. Barrera-Barrera Gabriela, Cucoch-Petraello-Rojas Camila, Martínez-Vera Ignacia, Neira-Pérez Marybel, Órdenes-Osorio Soledad, Sandoval-Rubilar Scarlett et al. Percepción de las vías del parto de mujeres en edad reproductiva: una revisión de la literatura. Rev. chil. obstet. ginecol. [Internet]. 2022 Abr [citado 2023 Jul 18] ; 87(2):122-136.
3. García Prieto DJ, Alonso Sánchez DJ, Casado Pérez DC, Cruz-Conde DMDC, Hernández DL, Martínez Chamorro DE. Complicaciones del puerperio: mecanismos fisiopatológicos y principales hallazgos radiológicos asociados . seram [Internet]. 18 de mayo de 2021 [citado 18 de julio de 2023];1(1).
4. Mendoza B Constanza, Saldivia Sandra. Actualización en depresión postparto: el desafío permanente de optimizar su detección y abordaje. Rev. méd. Chile [Internet]. 2015 Jul [citado 2024 Sep 19] ; 143( 7 ): 887-894.
5. Dominguez Mejias Maria, Depresión posparto. Importancia de la actuación de la matrona. A propósito de un caso. Rev Cientifico-Sanitaria [Internet]. 2021 [citado 2023 Jul 18]; 2021 5(4):38-46.
6. Benavides-Patricio. La depresión, evolución del concepto desde la melancolía hasta la depresión como enfermedad física. Rev PUCE. 2017;3528-8156(105):171-188.
7. Lara Ma, Patiño Pamela, Navarrete aura, Nieto Lourdes. Depresión Posparto, un problema de salud pública que requiere de mayor atención en México. Instituto Nacional de Psiquiatria. [Internet] 2019 [Citado el 18 de Julio 2023]
8. Intranet IMSS. Información en salud, indicadores datos y estadísticas, depresión por grupo etario 2023 [sitio web] 2023 [citado el 18 de Julio del 2023]
9. Ambriz-López, Roberto, Flores-Venegas, Sandra Rocío, Soria-López, Juan Antonio, Guerrero-González, Geraldina, Kawas-Morales, Adrián, Álvarez-Lozada Luis Adrián. Depresión posparto durante la pandemia de COVID-19. Ginecol. obstet. Méx. [revista en la Internet]. 2022 [citado 2023 Ago 02] ; 90( 1 ): 8-20.
10. Macías-Cortés Emma del C., Lima-Gómez Virgilio, Asbun-Bojalil Juan. Exactitud diagnóstica de la Escala de Depresión Posnatal de Edimburgo: consecuencias del tamizaje en mujeres mexicanas. Gac. Méd. Méx [revista en la Internet]. 2020 Jun [citado 2024 Sep 19] ;156( 3 ):202-208.
11. Fernández Vera Johalys Karina, Iturriza Natale Alejandra Teresa, Toro Merlo Judith, Valbuena Rosalba. Depresión posparto valorada mediante la escala de Edimburgo. Rev Obstet Ginecol Venez [Internet]. 2014 Dic [citado 2024 Sep 19] ; 74( 4 ): 229-243.
12. Manuel O, Teresa L, Itzel G, Sara M. Validez y seguridad de la escala de Depresión perinatal de Edimburgo de tamiz para detectar depresión perinatal. Perinatol Reprod Hum [Revista en la internet] 2008 [cited el 2023 Ago 02]; 22:195-202.
13. González-Gastélum César Dalí, Ávila-Gámez Luis Daniel, Briseño-Robles Claudia Iveth, Morales-García Norma Carolina, Becerra-Durand Ana Irais, Frías-Mendívil Mauricio. Depressive symptoms in pregnant women treated at the Hospital Infantil del Estado de Sonora. Salud Ment [revista en la Internet]. 2024 Feb [citado 2024 Sep 19] ; 47( 1 ): 13-22.
14. Abenova Madina, Myssayev ayan, Kanya Lucy, Turliuc Maria, Jamedinova Ulzhan. Prevalence of postpartum depression and its associated factors within a year after birth in Semey, Kazakhstan: A cross sectional study. Elsevier ScienceDirect [Internet] 30 de Junio 2022 [Citado el 18 de Julio del 2023]
15. Prevención, diagnóstico y manejo de la depresión prenatal y postparto en el primer y segundo niveles de atención. Guía de Práctica Clínica: Evidencias y Recomendaciones. México, CENETEC; 2021 [01 de Agosto del 2023].
Citation
Bray-Contreras B. and Serrano-García EA, Postpartum depression associated with the route of obtaining the newborn, ERSJ 2025,1(1) https://doi.org/00.0000/v0000000
Academic Editor: Alfonso Vallejos Paras, Received: 13 April 2025, Revised: 6 May 2025, Accepted: 11 May 2025, Published: 13 May 2025