Effectiveness of alcohol solutions at different concentrations as a disinfectant for hand hygiene
María de los Ángeles Lizbeth Muñiz Alvarado1, Luis Enrique Pérez Gómez2 Jesús Abraham Aguilar Campos2, Porfirio Felipe Hernández Bautista3, Guadalupe García Bracamontes1
1. Regional General Hospital No. 1, Ciudad Obregón 85110, Mexico. 2. High Specialty Medical Unit 08, Specialty Hospital, Ciudad Obregón 85120, Mexico. 3. Coordination of Quality of Supplies and Specialized Laboratories, Mexican Institute of Social Security, Mexico City 07760, Mexico.
Abstract
Introduction: Healthcare-associated infections are the leading cause of prolonged hospital stays, as well as leading cause of long-term disability, increased deaths, and increased costs. Hand hygiene has been a highly effective intervention in reducing healthcare-associated infections; however, the alcohol concentration range is very wide (60% to 95%), in line with WHO recommendations.Objetive: To evaluate the effectiveness of alcohol-based solutions at different concentrations as hand hygiene disinfectants for healthcare personnel and family members of patients at Regional General Hospital 1, Ciudad Obregón, Sonora.
Materials and methods: A quasi-experimental study was carried out which included health personnel working at the Regional General Hospital 1 and relatives of hospitalized patients in the different services (the caregiver), the hand hygiene technique was performed in vivo and in vitro to assess susceptibility according to the 5 most frequent microorganisms in Infections associated with health care and with a pattern of antimicrobial multi-resistance from March 1 to July 31, 2015.
Results: The reduction obtained with 90% alcohol solution was 97.79% at 10 seconds and 98.67% at 30 seconds, with 60% a reduction of 76.68% and 82.42% respectively; a greater reduction was observed with 90% alcohol solution and hand hygiene technique: 98.06% at 10 seconds and 99.20% at 30 seconds.
Conclusions: The 90% alcohol solution was the factor that showed statistical significance for both Gram positive and Gram-negative bacteria.
Keywords: Effectiveness, alcohol solutions, Healthcare-associated infections.
INTRODUCTION
A healthcare-associated infection (HAI) is a localized or systemic condition, resulting from an infectious agent or its toxins, contracted by a patient during treatment in a hospital or other healthcare facility and which was neither present nor in the incubation phase at the time of admission.1
Worldwide, it is estimated that more than 1.4 million people contract hospital-acquired infections; between 5% and 10% of patients admitted to hospitals in developed countries will contract one or more infections. In the United States of America (USA), one in every 136 hospitalized patients becomes seriously ill from a hospital-acquired infection, equivalent to 2 million cases and approximately 80,000 deaths annually.2 This generates an average cost ranging from $382.00 to $1,833.00 US per case; In Canada, the annual cost of nosocomial infections is $0.3 to $1 billion; in Germany, the annual cost is estimated at $0.3 to $0.6 billion. HAIs are the leading cause of prolonged hospital stays, as well as long-term disability, increased deaths, and increased costs.4 Several studies have shown that poor hand hygiene is the most common cause of HAIs.5, 6 Similarly, it has been observed that handwashing with alcohol-based solutions prevents the transmission of nosocomial pathogens by healthcare workers, as alcohols possess antimicrobial activity attributed to their ability to denature proteins.7, 8 Alcohol-based solutions, at concentrations of 60% to 95%, are more effective, while higher concentrations are less potent, as proteins do not denature easily in the absence of water. They also reduce hand hygiene time. They have been shown to have excellent in vitro germicidal activity against gram-positive and gram-negative bacteria, including multidrug-resistant pathogens, Mycobacterium tuberculosis, and several fungi. Some enveloped viruses, such as the Human Immunodeficiency Virus, Herpesvirus, Influenza, and Respiratory Syncytial Virus, are sensitive to alcohol. 7, 8 It is therefore important to practice proper hand hygiene to reduce healthcare-associated infections. Various guidelines recommend that handwashing be performed with alcohol-based solutions at a concentration of 60% for a period of 30 seconds to be effective. The World Health Organization even establishes guidelines for preparing alcohol-based solutions, thus ensuring greater effectiveness. 9, 10, 11 It is worth noting the rise in the use of alcohol-based solutions in recent years, as mentioned by Angeles et al. (2005) in their clinical trial conducted at the IMSS La Raza Medical Center (CMN la Raza), where they compared the effectiveness of using alcohol gel and the traditional hand disinfection technique in reducing CFUs on the hands of doctors and nurses, obtaining a CFU-Log10 reduction of 0.7 versus 1.53 (p≤0.01); observing that the nurses group had a greater reduction in CFUs-Log10 than the doctors (p<0.05). In 2004, at the Department of Medicine of the State University of Maringá, Brazil, Hernandes et al. compared the effectiveness of alcohol-based hand gel with traditional handwashing for the elimination of agents such as Acinetobacter baumannii, methylcylin-resistant Staphylococcus aureus, Escherichia coli, Enterococcus faecalis, Pseudomonas aeruginosa, and Candida albicans. They concluded that handwashing with liquid soap reduced the number of microorganisms by 93.83%, 100% povidone-iodine, and 99% alcohol-based hand gel. They also demonstrated that 4 of 6 microorganisms analyzed with the different disinfectants were removed. 13 On the other hand, Alvarado et al. (2008) studied the antiseptic capacity of two different brands of alcohol-based hand gel, without specifying the final alcohol concentration, and compared its effectiveness with a 70% liquid alcohol solution. They found that the greatest antimicrobial effects for both gels were obtained after 30 s and for liquid alcohol after 1 minute. An ANOVA distribution was used for statistical analysis and it was concluded that the alcohol presentation does not interfere with the percentages of bacterial reduction and the time for maximum bacterial inhibition is 30 s. 14 Kampf and Hollingsworth (2008) evaluated the bactericidal activity of an ethanol-based hand gel in 15 s and its efficacy against 11 gram-positive bacteria, 16 gram-negative bacteria, and 11 emerging bacterial pathogens. Each strain was evaluated in quadruplicate; They found that hand gel (85% ethanol) reduced 11 gram-positive and 16 gram-negative bacteria by more than 5 logs in 15 seconds and that it has a broad bactericidal spectrum. 15 Herruzo-Cabrera et al. (2001) studied the effects of various alcohol solutions on the resident and acquired microbiota, comparing them with conventional handwashing in vivo and in vitro. Significant differences were found in both designs. Handwashing barely modified the native or acquired microbiota (only 0.1 to <2 logs) and did not eliminate Staphylococcus aureus and gram-negative bacteria (34–23%; P > 0.05). However, N-duopropenide reduced the acquired microbiota by 5 logs and the native microbiota by more than 2 logs, as well as S. aureus and gram-negative bacteria (33–1.3%; P < 0.01).MATERIALS AND METHODS
The study was conducted at Regional General Hospital No. 1, located in Ciudad Obregón, Sonora. The study period ran from March 1 to July 31, 2015. A quasi-experimental, double-blind study was conducted with healthcare personnel and family members of patients who met the inclusion criteria.
The sample size was calculated and yielded 52 participants. The study included healthcare personnel (physicians, nurses, and residents) working at the Northwest National Medical Center in Ciudad Obregón, Sonora, as well as family members of hospitalized patients (only the caregiver) from departments with the highest incidence of healthcare-associated infections (internal medicine, gynecology and obstetrics, surgery, traumatology, orthopedics, pediatrics, and emergency departments). Individuals with product allergies, dermatitis, prior hand hygiene, family members other than the patient's caregivers, or visibly dirty hands were excluded, and samples contaminated during transport or planting were eliminated.
The dependent variable was hand disinfection effectiveness, and the independent variables were the use of alcohol-based hand sanitizers at different concentrations, sex, adverse reactions, hand hygiene technique recommended by the WHO, hand rubbing time, assigned service, type of worker, and pathogen isolated.
The study protocol was submitted to the local research committee, and written consent was obtained from study participants.
The alcohol-based hand sanitizer was prepared at different concentrations (60% and 90%) according to the WHO-recommended guidelines for the preparation of hand sanitizer formulations. This was carried out as follows: 96% ethanol (8333 ml) was poured into a 10-liter plastic bottle fitted with a screw-top cap, 3% hydrogen peroxide (417 ml) was added, and 98% glycerol (145 ml) was added using a measuring cylinder. The bottle was then filled to the 10-liter mark with sterile distilled water. Once the preparation was completed, it was immediately capped to prevent evaporation. The solution was mixed by gentle shaking, and the solution was distributed into 100-ml plastic containers. The bottles were quarantined for 72 hours to eliminate any spores present in the alcohol or bottles. Quality control was monitored using an alcohol breathalyzer.
Initially, a hand sample was taken with a swab moistened with 0.45% saline solution, rubbing it over the entire surface. The swab was then placed in Brain-Heart Infusion (BHI) broth. Subsequently, 2 ml of alcohol-based solution at 60% and 90% concentrations was applied to the hands, and hands were washed. Most healthcare personnel performed this procedure using the WHO-recommended technique, while patient family members did not. Samples were taken again 10 and 30 seconds after application. The collected samples were taken to the laboratory, incubated for 4 hours, and cultured using the mass plating technique with a 0.1 ml calibrated loop in base agar for CFU counting. For microorganism identification, samples were plated on blood agar, MacConkey agar, and mannitol salt agar. They were kept in incubation for 24 hours, at the end the colonies were isolated for identification by direct observation on a plate, as well as observation with a microscope and if necessary they were introduced to the VITEK 2. As a complement to the study, in vitro susceptibility tests were performed with a suspension of bacteria in a test tube with 0.45% saline solution as a diluent, it was verified that it had an optical density of 0.5 McFarland and dilutions 1:2, 1:4, 1:8, 1:16 and 1:32 were made with the different concentrations of alcohol solution (2 ml), the sample was homogenized by vortexing and the inhibition of strains was evaluated at 10s and 30s, a sample was taken with the calibrated loop extended on the plate, it was left to incubate for 24 hours and the CFU count was performed, the microorganisms were selected according to their development in cultures of hospitalized patients, the five most common or outbreak-causing pathogens (Acinetobacter baumannii complex, Klebsiella pneumoniae, Escherichia coli, Pseudomonas aeruginosa, and Stenotrophomona maltophila) were identified, and the pattern of antimicrobial multidrug resistance was established.
A form was created in Epi Info 7® for all participants, including healthcare personnel and family members of hospitalized patients. A univariate analysis was then performed, applying frequency and central tendency measures depending on the type of variable, as well as proportions for qualitative variables.
Quantitative variables were evaluated using ANOVA statistics. A bivariate analysis was also performed using the Mann-Whitney U test. For qualitative variables, the chi-square test was used. Risk assessment was performed using Hazard Ratio. Multivariate analysis was performed using Cox proportional hazards. The software used was STATA® and Epi Info 7®.
RESULTS
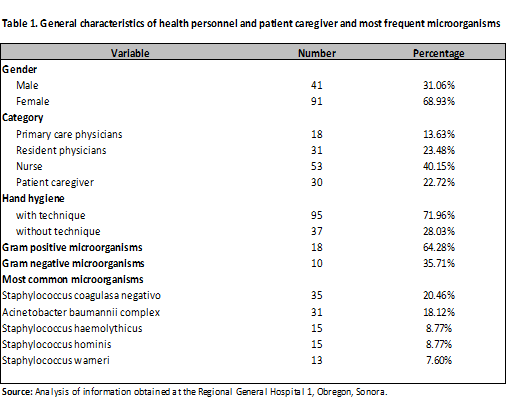
Data was collected from a total of 132 participants of both sexes over a five-month period. The study participants were 31.06% male and 68.93% female. The categories included were attending physicians (13.63%), resident physicians (23.48%), nurses (40.15%), and patient family members (caregivers) (22.72%). The alcohol-based hand sanitizer was applied in equal proportions to each study subject. Of the total participants, 71.96% performed hand hygiene using the WHO-recommended technique, and 28.03% did not (Table 1). According to microorganism development, 18 Gram-positive strains (64.28%) and 10 Gram-negative strains (35.71%) were isolated, totaling 171 bacteria. Among these strains, coagulase-negative Staphylococcus (20.46%) were isolated in order of frequency, followed by Acinetobacter baumannii complex (18.12%), Staphylococcus haemolyticus (8.77%), Staphylococcus hominis (8.77%), and Staphylococcus warneri (7.60%) (Table 1).
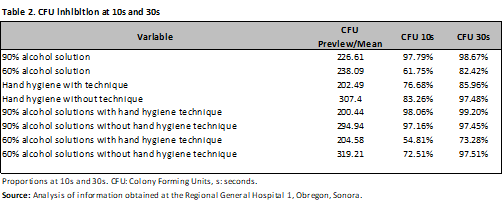
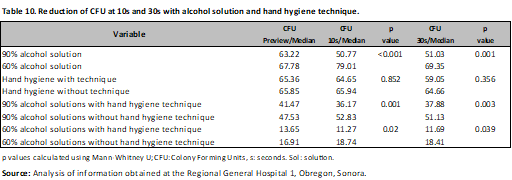
The reduction obtained with the 90% alcohol solution was 97.79% at 10 s and 98.67% at 30 s. The reduction obtained with the 60% solution was 76.68% and 82.42%, respectively. A greater reduction was observed with 90% alcohol solution using hand hygiene: 98.06% at 10 s and 99.20% at 30 s (Table 2).
Colony-forming unit inhibition was evaluated using analysis of variance (ANOVA), which compared the inhibition with 90% alcohol solution, obtaining a p < 0.001, with a mean of 226.61 CFU in the pre-culture, with development of 5 CFU at 10 s and 3.01 CFU at 30 s after application of the alcohol solution. When applied with 60% alcohol solution, a p = 0.03 was obtained, with a mean of 238.09 CFU in the pre-culture, 91.6 CFU at 10 s, and 41.85 CFU at 30 s (Table 3).
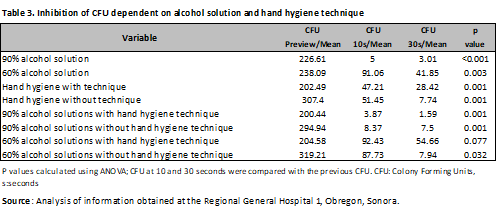
Regarding hand hygiene with the technique, a p < 0.001 was observed, with a mean of 202.49 CFU before, 47.21 CFU after 10 seconds, and 28.42 CFU after 30 seconds. When hand hygiene was performed without the technique, a p < 0.001 was observed, with a mean of 307.40 CFU before, 51.45 CFU after 10 seconds, and 7.74 CFU after 30 seconds (Table 3). Regarding the use of 90% alcohol solution with hand hygiene technique, a p < 0.001 was found with a mean of 200.44 in the previous, 3.87 at 10s and 1.59 at 30s, the same solution, but without technique presented a p < 0.001, with 294.94 CFU in the previous, 8.37 at 10s and 7.5 at 30s; A difference was noted with the 60% alcohol solution with the technique, as it presented a p=0.07, not being statistically significant with a mean reduction of 92.43 CFU at 10 s and 54.66 CFU at 30 s. However, without the technique, a p=0.03 was obtained, with a mean reduction of 87.73 at 10 s and 7.94 CFU at 30 s from a previous development of 319.21 CFU .
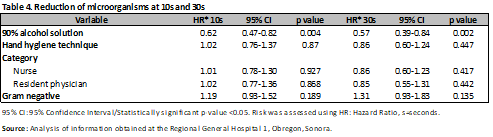
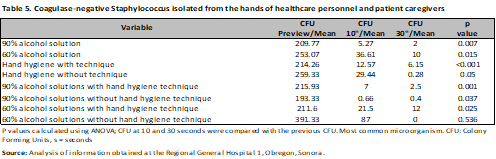
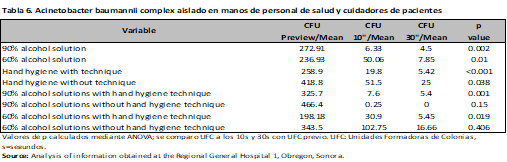
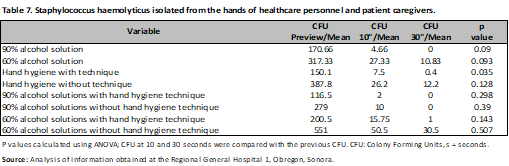
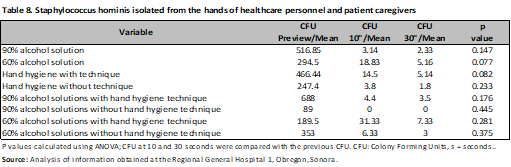
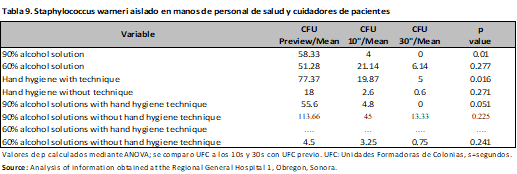
The risk was evaluated through Hazard Ratio (HR), observing that the application of 90% alcohol solution represents a protective factor for the development of microorganisms at 10s (HR 0.62; 95% CI, 0.47-0.82; p<0.001), with no difference with the hand hygiene technique. (HR 1.02; 95% CI, 0.76-1.37; p=0.87) a comparison was made between nurses and resident physicians, without showing differences between them (HR 1.01; 95% CI, 0.78-1.30; p=0.92) and (HR 1.02; 95% CI, 0.77-1.36; p=0.86), finally Gram-negative microorganisms were evaluated (HR 1.19; 95% CI, 0.93-1.52; p=0.18) (Table 4). The same was done at 30s, and again, the protective factor was found to be 90% alcohol solution (HR 0.57; 95% CI, 0.39-0.84; p < 0.001), hand hygiene technique (HR 0.86; 95% CI, 0.60-1.24; p = 0.44), category (nurses and medical residents) (HR 0.86; 95% CI, 0.60-1.23; p = 0.41) and (HR 0.85; 95% CI, 0.55-1.31; p = 0.44). There was no difference in Gram-negative bacteria (HR 1.31; 95% CI, 0.93-1.83; p = 0.13) (Table 4). In the analysis by microorganisms a difference was observed with alcoholic solution and hand hygiene technique mainly, as in the case of Acinetobacter baumannii complex with 90% and 60% alcoholic solution (previous CFU/mean 272.91; CFU 10s/mean 6.33; CFU 30s/mean 4.5; p<0.001), (previous CFU/mean 236.93; CFU 10s/mean 50.06 CFU 30s/mean 7.85; p=0.01) with and without hand hygiene technique (previous CFU/mean 258.90; CFU 10s/mean 19.8; CFU 30s/mean 5.42; p<0.001), (previous CFU/mean 418.8; CFU 10s/mean 51.5 CFU 30s/mean 25; p=0.03), having a similar behavior in the case of Gram positives (Tables 5-9).
A difference was observed in the Mann-Whitney U test regarding the use of alcohol-based hand rub (p < 0.001 at 10 s; p < 0.001 at 30 s) and the combination of alcohol-based hand rub with and without hand hygiene (p=0.003; p=0.039, respectively). This was not the case for the hand hygiene technique, where no difference was observed (p=0.356) (Table 10).
A chi-square test was performed to determine differences in the microbiota developed by healthcare personnel and patient caregivers. No differences in the development of microorganisms were observed with this method (p=0.10).
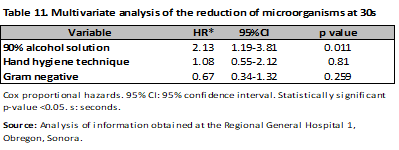
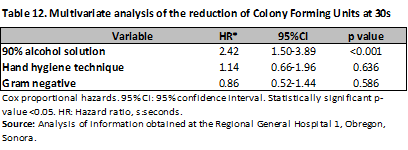
In the multivariate analysis performed using Cox proportional hazards, it was observed that the 90% alcohol solution reduced the bacterial load up to twofold more when rubbed for 30 s (HR of 2.13; 95% CI, 1.19-3.81; p = 0.01), while the hand hygiene technique had no association (HR 1.08; 95% CI, 0.55-2.12; p = 0.81) and Gram-negative bacteria were also not statistically significant (HR 0.67; 95% CI, 0.34-1.32; p = 0.25) (Table 11). When analyzing the CFU reduction at 30 s, a difference was only observed with the alcohol solution, with a HR of 2.42; 95% CI, 1.50-3.89; p < 0.001. This difference was corroborated in the multivariate analysis. No differences were observed for the remaining variables (Table 12).
It is worth mentioning that contaminated samples were excluded from the analysis. In vitro tests performed with the five main microorganisms that developed at Regional General Hospital 1 with a pattern of antimicrobial multidrug resistance, a significant reduction in CFU was observed with the 90% alcohol solution, which was greater at 30 s in most dilutions. This was the case with the 60% alcohol solution, where a smaller reduction was observed, especially in microorganisms such as Klebsiella pneumoniae and Acinetobacter baumannii complex .
DISCUSSION
The presence of HAIs represents a serious problem for patient safety, and their prevention should be a priority in healthcare institutions.3
The main objective of this study was to evaluate the effectiveness of alcohol-based solutions at different concentrations as a disinfectant for hand hygiene among healthcare personnel and patients' families. This was achieved by observing a reduction in CFUs with the use of 60% and 90% alcohol-based solutions. The latter was more effective, achieving a greater reduction within 30 seconds. This is in agreement with Kampf G and Ostermeyer C., who demonstrated the efficacy of alcohol-based solutions at concentrations between 60% and 95%, conferring efficacy against Gram-positive and Gram-negative bacteria.7
Similarly, a considerable reduction in CFU was observed when performing hand hygiene in 10 s, which is slightly lower than the WHO recommendation and the time observed in the Kampf and Hollingsworth study, which evaluated the bactericidal activity of an ethanol-based hand gel in 15 s, finding efficacy against 11 gram-positive bacteria, 16 gram-negative bacteria, and 11 emerging bacterial pathogens. 15 Therefore, hand hygiene is the main measure whose effectiveness in preventing HAIs has been demonstrated. Such is the case of Angeles et al. in their clinical trial, which demonstrated the effectiveness of using alcohol gel for hand disinfection by reducing CFUs in the hands of doctors and nurses, obtaining a Log10 CFU reduction of 1.53 (p < 0.01). They observed that the nurses had a greater Log10 CFU reduction than the doctors (p < 0.05), which is consistent with the results of this study regarding CFU reduction. However, there is a discrepancy regarding the reduction in the categories since no difference was observed between them.12
In the bivariate analysis, a difference was observed with the alcohol-based hand sanitizer, but this was not the case for the hand hygiene technique.
In the multivariate analysis, a difference was observed only with the alcohol-based hand sanitizer, both for the reduction of microorganisms (HR: 2.13; 95% CI, 1.19–3.81) and for Colony-Forming Units (HR: 2.42; 95% CI, 1.50–3.89).
In this study, a 97.79% reduction was observed at 10 seconds, with a greater reduction achieved at 30 seconds, reaching 98.67% with the 90% alcohol-based hand sanitizer. This correlates with the results of Hernandes in Brazil, who compared the effectiveness of alcohol-based hand sanitizer with traditional handwashing. They concluded that the alcohol-based hand sanitizer reduced the risk of up to 99% and significantly removed Gram-negative bacteria. There are studies such as that of Alvarado et al., which investigated the antiseptic properties of alcohol gel without specifying the concentration and 70% liquid alcohol. They found a greater effect with alcohol gel after 30 seconds and with liquid alcohol up to one minute after application. This aspect is not consistent with this study, since a significant reduction was observed after 10 seconds; however, this could have been due to the lower ethanol concentration than the one used in this study. 14
In vitro tests, a greater reduction in CFU was observed with the 90% alcohol solution than with the 60% solution, which is consistent with what Herruzo-Cabrera demonstrated in the comparative study of conventional handwashing and alcohol-based solutions in vivo and in vitro, where a greater reduction in CFU was found with the latter, including Gram-negative microorganisms. The use of alcohol gel offers several benefits, including faster hand hygiene, fewer adverse reactions (which occurred in only 2% of participants in this study), immediate availability at the patient's bedside, and lower cost.
This work provides a basis for future research to evaluate antimicrobial resistance and sensitivity in vivo hand hygiene studies, as well as serving as a basis for reconsidering proper hand hygiene.
REFERENCES
1.Organización Mundial de la Salud. Carga mundial de infecciones asociadas a la atención sanitaria [Internet]. México: OMS; [2013, acceso el 10 de septiembre 2014]. Disponible en: http://www.who.int/gpsc/country_work/burden_hcai/es/
2.Organización Mundial de la Salud. Una atención limpia es una atención más segura [Internet]. México: OMS; [13/10/13, acceso el 19 de septiembre 2014]. Disponible en: http://www.who.int/gpsc/es/
3.Organización Mundial de la Salud. News and top stories [Internet]. África: OMS; [04/2009, acceso en enero 2015].Disponible en:http://www.who.int/en/
4.World Health Organization. Guide line on hand hygiene in health care, first global patient safety challenge clean care is safer care [Internet]. Suiza: WHO; [2009, acceso en noviembre 2014].Disponible en: http://apps.who.int/iris/bitstream/10665/44102/1/9789241597906_eng.pdf
5.Babiarz L, Savoie B, McGuire M, McConnell L, Nagy P. Hand sanitizer- dispensing door handles increase hand hygiene compliance: a pilot study. Am J Inf Control. [Internet]. 2014 [Consultado en octubre 2014]; 42(4) [443-445]. Disponible en:http://www.sciencedirect.com/science/article/pii/S0196655313013679
6.Abaza AF, Amine AE, Hazzah WA. Comparative study on efficacy of different alcohol hand rubs and routine hand wash in a Health-Care Setting, Alexandria, Egypt. J Egypt Public health Assoc. [Internet].2010 [Acceso en noviembre 2014]; 85(5-6) [273-282]. Disponible en: http://www.ncbi.nlm.nih.gov/pubmed/22054102
7.Kampf G, Ostermeyer C. Efficacy of alcohol-based gels compared with simple hand wash and hygienic hand desinfection. J Hosp Infec. [Internet].2004 [Acceso en octubre 2014]; 56(Supl 2)[s13-s15]. Disponible en: http://www.sciencedirect.com/science/article/pii/S0195670103005127
8.Organización Central Osakidetza. Guía de higiene de manos para profesionales sanitarios [Internet]. España; Gobierno Vasco; [2009, acceso en octubre 2014]. Disponible en:http://www.hospitalcruces.com/documentos/campanas/GUIA%20HIGIENE%20OSAKIDETZA.pdf
9.Parienti JJ, Thibon P, Heller R, Le Roux Y, von Theobald P, Bensadoun H et al. Hand-rubbing with an aqueous alcoholic solution vs traditional surgical hand-scrubbing and 30-day surgical site infection rates: a randomized equivalence study. JAMA [Internet]. 2002 [Acceso en enero 2015]; 288(6)[722- 727]. Disponible en:http://jama.jamanetwork.com/article.aspx?articleid=195187
10.Organización Mundial de la Salud Guía para la elaboración a nivel local: formulaciones recomendadas por la OMS para la desinfección de manos [Internet]. España: OMS; [2012,acceso en diciembre 2014].Disponible en http://www.who.int/gpsc/5may/tools/ES_PSP_GPSC1_GuiaParaLaElaboracion LocalWEB-2012.pdf?ua=1
11.Center for Disease Control and Prevention. Guideline for hand hygiene in health-care settings: recommendations of the healthcare infection control practices advisory committee and the HICPAC / SHEA / APIC / IDSA hand hygiene task force [Internet]. EEUU: CDC; [25/19/2002, Acceso en enero 2015]. Disponible en: http://www.cdc.gov/mmwr/PDF/rr/rr5116.pdf
12.Angeles U, Molinar F, Anaya V, López M. Efectividad de la aplicación de alcohol gel en la higiene de las manos de enfermeras y médicos. Rev Enferm Inst Mex Seguro Soc. 2005; 13(1):15-21.
13.Daniel-Hernandes SE, de MelloII AC,Jordão-Sant'Ana AJ, Sarto-Soares V,Cassiolato V,Botelho-Garcia L, et al.The Efectiviness of alcohol gel and other hand-cleansing agents against, important nosocomial pathogens. Brazilian J Microbiol. [Internet]. 2004 [acceso en noviembre 2014]; 35(1)[33- 39]. Disponible en: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1517- 83822004000100005
14.Alvarado D, García JD, Arias-Echandi ML. Evaluación de la efectividad del alcohol gel en la desinfección de manos y su estabilidad a través del tiempo. Rev Biomed. [Internet]. 2010 [Acceso en enero 2015]; 21(1)[29-31]. Disponible en: http://dialnet.unirioja.es/servlet/articulo?codigo=3992684
15.Kampf G, Hollingsworth G. Comprehensive bactericidal activity of an ethanol- based hand gel in 15 seconds. AnClinMicrobiolAntimicrob. [Internet].2008 [acceso en diciembre 2014]; 7(2). Disponible en:http://www.ann- clinmicrob.com/content/7/1/2
16.Herruzo-Cabrera R, García-Caballero J, Fernández-Aceñero MJ. A new alcohol solution (N-Duopropenide) for hygienic (or routine) hand desinfection is more useful than classic handwashing: in vitro and in vivo studies in burn and other intensive care units. Burns. [Internet].2001 [Acceso en enero 2015]; 27(7)[747-752].Disponible en:http://www.sciencedirect.com/science/article/pii/S0305417901000134
17.Gobierno de la República, Instituto Mexicano del Seguro Social.Modelo Institucional para prevenir y reducir las infecciones nosocomiales. [Internet]. México: IMSS; [2013, Acceso en diciembre 2014]. Disponible en: http://es.scribd.com/doc/231519675/MODELO-INSTITUCIONAL-PREVENIR- Y-EDUCIR-INFECCIONES-NOSOCOMIALES-pdf#scribd
Citation
Muñiz Alvarado MAL et al. Effectiveness of alcohol solutions at different concentrations as a disinfectant for hand hygiene ,ERSJ 2026,1(4) 175 -188
Academic Editor: Yadira Pérez Andrade Received: 2025 may 22 Revised: 2025 may 22 Accepted: 2025 may 22 Published: 2026 april 18