Impact of healthcare-associated infections on hospital costs, length of stay, and mortality
Alejandra Medina-González and Carmen Alicia Ruíz-Valdez
Instituto Mexicano del Seguro Social. Hospital General Regional No.1, Av. Vicente Guerrero, Bellavista, 85110, Obregón, Sonora, México
Abstract
Introduction: Healthcare-associated infections are a public health problem, mainly related to invasive medical procedures, as well as the condition of patients, such as those requiring admission to intensive care, increasing morbidity and mortality rates, and consequently increasing hospital costs by delaying patient discharge.Objetive: To identify the impact of healthcare-associated infections (HAIs) on hospital costs, length of stay, and mortality.
Materials and methods: An observational, descriptive, cross-sectional prevalence study was conducted.
Results: A total of 1791 infection records and 24 analyses were performed, revealing a predominance in males (55.6%). The predominant age groups were those over 65 years and under 1 year old. A correlation was found between healthcare-associated infections (HAIs) and extended hospital stay (R 0.932), hospital costs (R 0.734), and mortality (R 0.049). The infection that generated the highest costs due to extended stay was ventilator-associated pneumonia (VAP) ($229,883,992.00).
Conclusions: A relationship was found between costs and healthcare-associated infections (HAIs), as well as with the resulting overstay. No relationship was found between deaths caused by the increase in HAIs. Invasive procedures continue to be a key factor in the costs generated.
Keywords: HAIs, INOSO, costs, overstay, mortality.
INTRODUCTION
The World Health Organization (WHO) defines healthcare-associated infections (HAIs) as “infections that affect a patient during care in a hospital or other healthcare facility, which were not present or incubating at the time of admission. They also include infections acquired in the hospital, but which manifest after discharge.” HAIs, also known as nosocomial or hospital-acquired infections, are the most frequent adverse event during the provision of medical care, and can affect both patients and healthcare personnel.1,2
The Mexican Official Standard NOM-045-SSA2-2005, for the epidemiological surveillance, prevention, and control of nosocomial infections, describes them as a major problem of clinical and epidemiological importance because these infections impact morbidity and mortality rates, as well as directly complicating patient care costs.4
WHO reports show that more than 1.4 million people worldwide contract hospital-acquired infections. In developed countries, the prevalence of patients who acquire at least one healthcare-associated infection (HAI) during their hospitalization ranges from 5% to 10%, while in developing countries it varies between 5.7% and 19.1%, reaching a proportion greater than 25% of affected patients in some countries. 2
General estimates of the impact of HAIs contribute to understanding their magnitude and potential consequences. European estimates indicate that HAIs cause 16 million days of excess hospital stay and 37,000 attributable deaths annually.7 In Mexico, HAI-related mortality in secondary and tertiary care institutions is 43.8%, while the WHO estimates that 450,000 healthcare-associated infections occur in Mexico, causing 32 deaths per 100,000 inhabitants per year.2
In Intensive Care Units (ICUs), the situation is even more complex due to the proportion of patients with invasive devices and their critical condition, which often requires the use of broad-spectrum antibiotics, antacids, parenteral nutrition, or other patient-specific factors such as pre-existing comorbidities that have been associated with a higher risk of HAIs. 8,9
Regarding the risk that healthcare-associated infections (HAIs) contribute to prolonged hospital stays, in Mexico this risk ranges from 5.9 to 9.6 days and, moreover, increases the probability of death by up to 6.9%, which implies a considerable increase in hospital costs.2,17
HAIs also represent a significant economic impact on healthcare facilities and on the cost of healthcare at the national level. Members of the Infection Prevention and Control (IPC) team must understand the financial burden of HAIs and be able to assess the savings that a given preventive intervention would represent.8,10 Measuring the financial impact of an HAIs on healthcare services can be difficult. However, hospital-acquired infections can have various economic consequences, from delaying patient discharge, which leads to higher occupancy of hospital beds, to increasing the cost of antimicrobial treatment and other interventions that the patient may require. They require greater use of diagnostic aids, increase costs in terms of infection prevention and control, and are often subject to legal proceedings.11,12
At the Mexican Social Security Institute, HAIs have various systems that support the process of collecting and analyzing information for the notification of probable, confirmed, and discarded HAIs, which are the Hospital Epidemiological Surveillance Unit (UVEH); the online platform for nosocomial infections (INOSO); and the system for adverse events, near misses, and sentinel events related to the Infection Prevention and Control system (VENCER II). The process and outcome indicator control panel, as well as the hospital committees where the results and functionality reports of the Committee for the Detection and Control of Healthcare-Associated Infections (CODECIAAS) are evaluated.8
The Official Gazette of the Federation, according to its latest update for 2023, presents the unit costs per level of medical care for the IMSS (Mexican Social Security Institute), establishing the cost per patient day in hospitalization and incubator at $11,919.00 each. The cost per patient day in intensive care is $62,705.00, the cost of wound care is $358.00, clinical laboratory tests are $152.00, radiodiagnostic studies are $517.00, surgical interventions are $38,830.00, and patients on mechanical ventilation are $44,953.00 per day.
The objective of the study was to understand the impact of HAIs on hospital costs, length of stay and mortality at Regional General Hospital No. 1 Ciudad Obregón, Sonora.
MATERIALS AND METHODS
The study was conducted at the Mexican Social Security Institute (IMSS): Regional General Hospital No. 1, Ciudad Obregón, Sonora, using an observational, descriptive, cross-sectional (prevalence) design. The study period was from December 26, 2017, to December 25, 2019.
The dependent variables were hospital costs, length of stay, and mortality, while the independent variable was healthcare-associated infections (HAIs).
The monthly analyses of HAIs reported by the Epidemiological Surveillance Unit of Regional General Hospital No. 1, Ciudad Obregón, Mexican Social Security Institute, were studied for the period of December 26, 2017, to December 25, 2019, totaling 1,791 infections. The monthly analyses included records of the number and type of HAIs, number of patients with HAIs, length of stay due to HAIs, monthly expenditures related to length of stay, and HAI-related mortality.
This represents the total number of infection records from the 24 censuses during the established period (1,791).
Data was obtained through a review of monthly analyses and the INOSO platform at Regional General Hospital 1, during the study period, totaling 1,791 infections, supplemented with information obtained from the Official Gazette of the Federation (DOF).
Inclusion criteria were records of patients with hospital-acquired infections, registered monthly on the INOSO platform; records of patients of both sexes; records of patients regardless of age; monthly analyses with monthly expenditures for hospitalizations and therapies; records of length of stay due to healthcare-associated infections (HAIs); and records of mortality associated with HAIs.
Exclusion criteria were records of patients with hospital-acquired infections imported from other units; records of patients with infections ruled out as healthcare-associated; monthly analyses without calculated monthly expenditures; and monthly analyses without records of mortality associated with HAIs. Exclusion criteria included patient records with incomplete data in the INOSO platform registry and incomplete monthly analyses.
The data were analyzed by reviewing sex, age, type of infection, length of hospital stay with infection (excess stay), costs associated with excess stay, and deaths. Costs, excess stay, and mortality (death due to or with HAIs) were considered dependent variables, while healthcare-associated infections were considered independent variables.
All information for the study was collected and recorded in a database created using a Microsoft Excel spreadsheet, which included the study variables as well as any supplementary information of interest. Once the database was completed, the analysis was performed using SPSS (Statistical Package for the Social Sciences) version 25. The results are presented in tables and graphs, along with their simultaneous interpretation.
For descriptive statistics, qualitative variables were summarized using frequency and percentage measures, while quantitative variables were summarized using measures of central tendency (mean, minimum, and maximum values) and measures of dispersion (standard deviation).
For inferential statistics, normality tests were performed. The risk of mortality with healthcare-associated infections (HAIs), sex, and type of infection was analyzed, as well as the risk of HAIs in relation to type of infection by sex and overstay in relation to the number of HAIs. Associations for qualitative variables were assessed using the Chi-square test (2); for quantitative variables, Student's t-test or Mann-Whitney U test was used, as appropriate.
For the quantitative variables of hospital overstay, costs associated with healthcare-associated infections (HAIs), and deaths, linear correlation and coefficient of determination were calculated, as well as HAI overstay by area of presentation, HAI costs by area, costs of overstay by area, and costs by type of infection. A 95% confidence level and a statistical significance level of 5% (p < 0.05) were considered.
This study was conducted in accordance with the ethical guidelines for health-related research involving human subjects developed by the Council for International Organizations of Medical Sciences (CIOMS) in collaboration with the World Health Organization, published in 2017. The local research committee granted the following registration number: R-2023-2601-072.
RESULTS
An observational, descriptive, analytical, retrospective, and cross-sectional study was conducted. Of a total of 1954 records, 1791 met the inclusion, exclusion, and elimination criteria. Additionally, 24 monthly analyses were performed to obtain supplementary data.
Table 1 presents the general characteristics of the population. Regarding the distribution of cases by sex, males predominated, representing 55.67% (997) of the observations, while females represented 44.33% (794) of the cases. Frequencies were obtained by age group, showing that the largest group was those 65 years and older, comprising 37.2% (666), followed by those under 1 year old, comprising 17.2% (308). The 25-44 age group represents 9.0% (161), followed by the 50-59 age group with 8.4% (150) and the 1-4 age group with 7.4% (132). Next are the 60-64 age group with 6.5% (116) and the 5-9 age group with 5% (89). Less frequently represented are the 10-14 age group with 3.2% (58), the 45-49 age group with 2.9% (52), the 20-24 age group with 2.0% (36), and the 15-19 age group with 1.3% (23). The frequency of healthcare-associated infections studied is also described, with the most frequent being "Other" at 54.7% (979 cases), followed by ventilator-associated pneumonia (VAP) at 15.0% (269 cases), urinary tract infection (CAUTI) at 12.6%, surgical site infection (SSI) at 9.5% (170 cases), and central venous catheter-related infection ( CLABSI) at 8.1% (146 cases).
Regarding the age of the participants, Table 2 describes the age range, from 0 years to 102 years, with a mean of 43.40 years and a standard deviation of ±32.428 (SD).
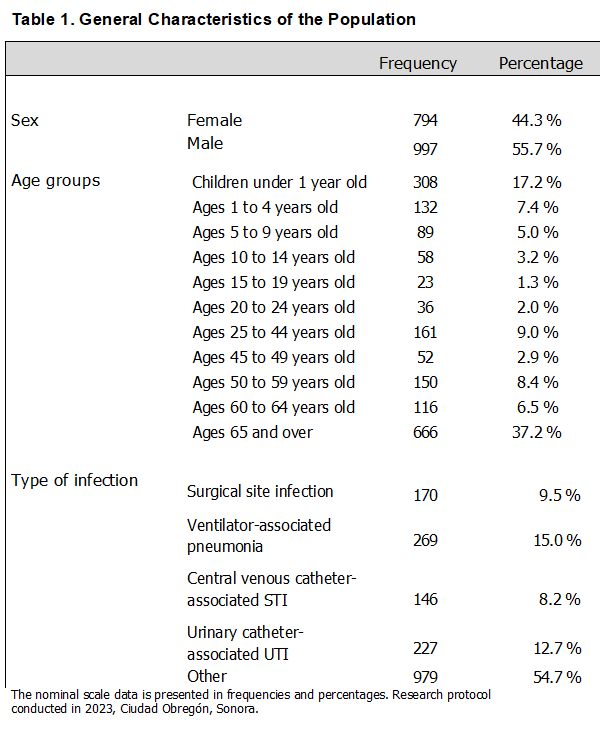

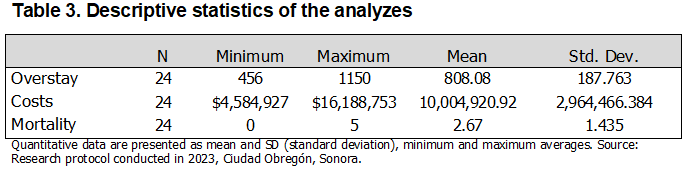
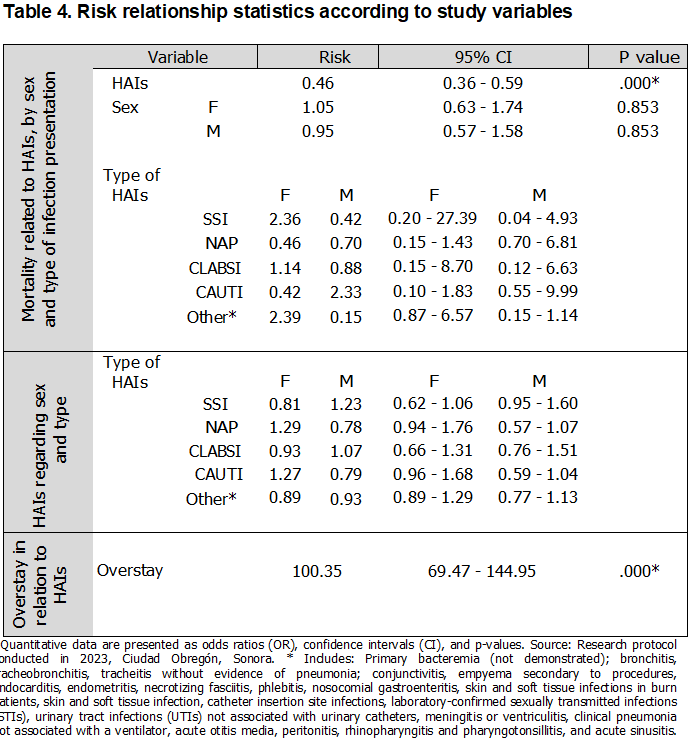
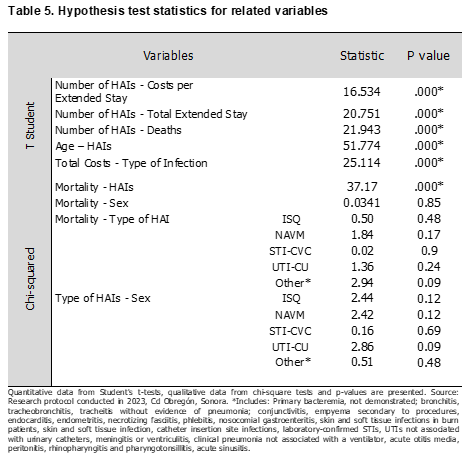
Table 3 describes the descriptive statistics analyzed monthly regarding hospital overstay, with a minimum of 456 and a maximum of 1150 days, and a mean of 808.08 days (±187.763 SD). Monthly costs for healthcare-associated infections (HAIs) ranged from a minimum of $4,584,927 to a maximum of $16,188,753, with a mean of $10,004,920.92 (±2964,466.384 SD). HAI-related deaths ranged from a minimum of 0 to a maximum of 5, with a mean of 2.67 (±1.435 SD). Regarding the risks associated with the variables, these can be observed in Table 4. The risk of mortality from HAIs was found to be an OR of 0.46 (p < 0.001). Mortality by sex showed an OR of 1.05 for females and an OR of 0.95 for males (p = 0.853, both sexes). Regarding mortality by type of HAIs and sex, the risk of developing a surgical site infection (SSI) was OR 2.36 in females and OR 0.42 in males (p = 0.17 for both sexes). The risk of developing ventilator-associated pneumonia (VAP) was OR 0.46 in females and OR 0.70 in males (p = 0.89, both sexes). The risk of developing a cardiovascular infection (CVI) was OR 1.14 in females and OR 0.88 in males (p = 0.89, both sexes). Regarding the association between the development of CAUTI in females, an OR of 0.42 was found for females and an OR of 2.33 for males (p=0.24, both sexes). For the risk of developing another infection, an OR of 2.39 was found in females and an OR of 0.15 in males (p=0.09, both sexes). Similarly, Table 4 presents the risks with respect to the type of HAIs according to sex, where SSI showed an OR of 0.81 for females and an OR of 1.23 for males (p=0.12); as for VAP, it presented an OR of 1.29 for females and an OR of 0.78 for males (p=0.12). Regarding the risk of developing CLABSI, an OR of 0.93 was found for females and an OR of 1.07 for males (p=0.69). For CAUTI, an OR of 1.27 was found for females and an OR of 0.79 for males (p=0.09); for the variable "Other," an OR of 0.89 was found for females and an OR of 0.93 for males (p=0.48). Regarding the relationship between the number of HAIs and overstay, an OR of 100.35 was found (p<0.0001). Table 5 presents the hypothesis tests where the relationship between the number of HAIs and overstay costs was sought, yielding a t-value of 16.534 (p<0.0001); regarding the number of HAIs and overstay, a t-value of 20.751 was found (p<0.0001). The relationship between the number of HAIs and mortality yielded a t-value of 21.943 (p<0.000). The age of presentation was associated with the number of HAIs, with a t-value of 51.774 (p<0.0001), and the costs by type of infection showed a t-value of 25.114 (p<0.0001). Likewise, an association was sought between mortality and number of HAIs, finding a 2 of 37.17 (p<0.000), mortality and sex with a 2 of 0.0341 (p=0.850), mortality by type of infection where SSI showed 2 of 0.50 (p=0.480), VAP with 2 of 1.84 (p=0.170), CLABSI with 2 of 0.02 (p=0.900), CAUTI with 2 of 2.94 (p=0.240) and Other with 2 of 2.94 (p=0.090). Regarding the association between the type of infection and sex, the following was found: SSI 2 =2.44 (p=0.122), NAVM 2 of 2.42 (p=0.120), CLABSI 2 =0.16 (p=0.690), CAUTI 2 =2.86 (p=0.090) and Other 2 =0.51 (p=0.480).
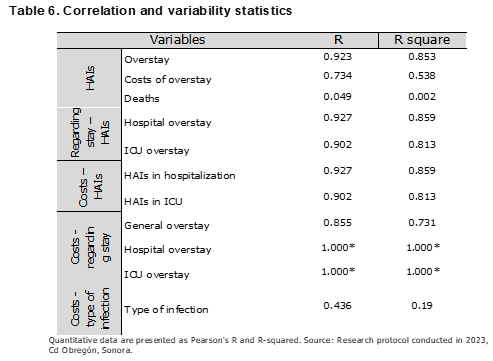
The correlation and variability are determined in Table 6, where the variables number of HAIs and overstay have a Pearson R of 0.923 and R2 of 0.853; the number of HAIs and costs due to overstay R 0.734 and R2 0.538; the number of HAIs and deaths R 0.049 and R2 0.002; overstay due to HAI in hospitalization R 0.927 and R2 0.859 and in overstay in ICU with R 0.902 and R square 0.813. Regarding the costs due to HAIs according to the area, for hospitalization an R 0.927 and for ICU an R 0.902 and R2 0.813. Regarding the relationship between costs and the excess stay generated, an R of 1.000 and an R2 of 1.000 were found for hospitalization, an R of 1.000 and an R square of 1.000 for ICU, while for general excess stay an R of 0.855 and an R square of 0.731. Finally, the relationship between costs and types of infection presented an R of 0.436 and an R2 of 0.190.
DISCUSSION
As Scott, Culler, and Rask (2019) state, healthcare-associated infections (HAIs) lead to increased costs due to prolonged hospital stays, the need for diagnostic tests, and hospital bed occupancy, among other factors. However, although this topic has been previously studied, it remains an area of opportunity for comprehensive care and addressing the changes it can generate in a hospital.11 According to our study, regarding age groups, the predominant group is those over 65 years old (37.2%), followed by those under 1 year old (17.2%). This indicates that the highest incidence of HAIs is found at the extremes of life, which could be associated with complications such as chronic diseases or prematurity in the case of newborns. According to the types of infection, based on the established variables, the predominance is found in Other with 54.7%, followed by VAP with 15% and UTI with 12.7%. However, considering that the study included in the variable “Other” all HAIs that did not have a history of an invasive procedure, it could be considered that the value is biased by the number of HAIs included in a single variable, so in reality VAP occupies first place, followed by CAUTI, determining that the greater presence of infections is associated with a previous invasive procedure, as mentioned by Perozo, Castellano González and Gómez Gamboa (2020), according to their study.6
In the development of the hypothesis tests, a student's t-test was performed where statistical significance was found in related variables. On the other hand, a statistically significant chi-square test (2) was found for mortality and HAIs (0.000*), which contrasts with the calculated odds ratio (OR = 0.46), which is also statistically significant, indicating no association between mortality and HAIs. The remaining associated variables did not show statistical significance in this study.
The relationship between HAIs variables and hospital costs, length of stay, and mortality was analyzed using linear correlation and the coefficient of determination to assess variability. The association between HAIs variables and hospital costs showed a strong, positive linear correlation (Pearson's R 0.734), indicating that costs increase proportionally with HAIs incidence. Similarly, 53.8% of the cost variability can be explained by the occurrence of HAIs. The relationship between HAIs variables and length of stay also showed an extremely strong, positive linear correlation (Pearson's R 0.923), indicating that length of stay increases proportionally with HAIs incidence. Furthermore, 85.3% of the variability in length of stay can be explained by the number of HAIs. In contrast, the relationship between HAIs and mortality showed a very weak correlation (Pearson's R 0.049), considering that R=0 means that there is no linear correlation, and the variability was 2%, which means that the model does not explain any variability; this contrasts with what was described by Barrasa Villar, Aibar Remón et al. (2017), where they established a significant relationship in the three variables studied.17 Ortiz Mayorga, Pineda Rodríguez, Dennis and Porras (2018), describe in their study the relationship between the cost of HAIs management and prolonged stay prior to its appearance, as described in this study where a strong linear correlation (Pearson's R 0.855) was found between general overstay and the costs for it, explaining that as overstay increases, hospital costs also increase, with a variability of 73.1%. Likewise, a comparison was made between hospitalization and ICU areas, where the relationship of both with overstay showed a perfect linear correlation with 100% variability, explaining that increased overstay increases hospital costs. Furthermore, the relationships between overstay and total HAIs, and HAIs costs by area, showed an extremely strong linear correlation (Pearson's R 0.927) for hospitalization with 85.9% variability for both relationships, and a strong linear correlation (Pearson's R 0.902) for ICUs with 81.3% variability for both relationships, indicating that as HAIs increase, overstay increases, and increased HAIs increase costs.
Regarding the relationship between costs and the type of infection, a moderate linear correlation was found (Pearson's R 0.436) with a variability of 19%, indicating that costs cannot be explained by the type of infection. The main objective of this research was to determine the impact of healthcare-associated infections (HAIs) on hospital costs, length of stay, and mortality at Regional General Hospital No. 1 in Ciudad Obregón, Sonora. The study period prior to the COVID-19 pandemic (2020 to 2023) was chosen to minimize bias. The analysis revealed that HAIs were more prevalent in males (55.6%) than in females, with ventilator-associated pneumonia (VAP) being the most common infection (15.08%), followed by urinary tract infections (CAUTI) (12.62%). The results obtained demonstrate that the increase in HAIs significantly impacts costs and length of stay, regardless of the area of presentation, as there is a positive correlation between the two. However, although mortality is related to HAIs, it was not demonstrated that the increase in HAIs impacts mortality itself.
REFERENCES
1. Ministry of Health. Manual for the Implementation of Action Packages to Prevent and Monitor Healthcare-Associated Infections (HAIs) [Online]. Mexico: Ministry of Health; 2019, [Accessed December 29, 2022]. Available from: http://www.calidad.salud.gob.mx/site/editorial/docs/manualIAAS.pdf
2. Marlenne I, Salgado R. Frequency of healthcare-associated infections in the main information systems of Mexico. CONAMED. 2018; 3(17).
3. Pan American Health Organization. Prevention and control of healthcare-associated infections [Online]. USA: PAHO; 2017, [Accessed December 29, 2022]. Available at: https://iris.paho.org/bitstream/handle/10665.2/51447/9789275319543_spa.pdf?sequence=1&isAllowed=y
4. Official Mexican Standard for the epidemiological surveillance, prevention, and control of nosocomial infections. NOM-045-SSA2-2005. Official Gazette of the Federation. (November 20, 2009).
5. Ovalle-Luna OD, Cuevas-García CF, Vázquez-Vázquez JA, Ordoñez-Alemán E, De Hilario-Alonso SO, et al. Risk of mortality from nosocomial infection in a tertiary care hospital. Rev Med IMSS. 2017; 55(5): 350-356.
6. Perozo A, Castellano-González MJ, Gómez-Gamboa LP. Healthcare-associated infections. Enferm Investig. [Internet]. 2020 [Accessed December 29, 2022];5(2):48-61. Available from: https://revistas.uta.edu.ec/erevista/index.php/enfi/article/view/877
7. World Health Organization. Report on the burden of endemic health care-associated infection worldwide [Online]. Switzerland: WHO; 2011, [Accessed December 29, 2022]. Available from: https://www.who.int/publications/i/item/report-on-the-burden-of-endemic-health-care-associated-infection-worldwide
8. Mexican Social Security Institute. Technical guide for the organization of epidemiological surveillance, prevention, and control of healthcare-associated infections. Mexico: IMSS; 2019.
9. Shrestha SK, Trotter A, Shrestha PK. Epidemiology and Risk Factors of Healthcare-Associated Infections in Critically Ill Patients in a Tertiary Care Teaching Hospital in Nepal: A Prospective Cohort Study. Infect Dis (Auckl). 2022. doi: 10.1177/11786337211071120
10. Benenson S, Cohen MJ, Schwartz C, Revva M, Moses AE, Levin PD. Is it financially beneficial for hospitals to prevent nosocomial infections? BMC Health Serv Res. 2020; 20(1):653.
11. Scott RD 2nd, Culler SD, Rask KJ. Understanding the economic impact of healthcare-associated infections: A cost perspective analysis. J Infus Nurs. 2019; 42(2):61–9.
12. Manoukian S, Stewart S, Dancer S, Graves N, Mason H, McFarland A, et al. Estimating excess length of stay due to healthcare-associated infections: a systematic review and meta-analysis of statistical methodology. J Hosp Infect 2018; 100:222–35.
13. Chamber of Deputies. Nosocomial infections represent a significant cost to public finances [Online]. Mexico: Chamber of Deputies; 2019, [Accessed December 29, 2022]. Available from: http://www5. diputados.gob.mx/index.php/esl/Communication/Bulletins/2019/April/12/1443-Nosocomial-infections-represent-a-great-cost-for-public-finances
14. Pan American Health Organization. Epidemiological surveillance of healthcare-associated infections. Module III: Information for managers and senior staff. Washington, DC: PAHO; 2012.
15. General Directorate of Epidemiology. Manual of standardized procedures for hospital epidemiological surveillance. Mexico: Ministry of Health; 2016.
16. Agreement number ACDO.AS3.HCT.251022/299.P.DF issued by the Honorable Technical Council, in its ordinary session of October 25, 2022, regarding the approval of the unit costs per level of medical care updated to 2023. Official Gazette of the Federation (November 11, 2022).
17. Barrasa-Villar JI, Aibar-Remón C, Prieto-Andrés P, Mareca-Doñate R, Moliner-Lahoz J. Impact on morbidity, mortality, and length of stay of hospital-acquired infections by resistant microorganisms. Clin Infect Dis [Internet]. 2017;65(4):644–52.
18. Page B, Klompas M, Chan C, Filbin MR, Dutta S, McEvoy DS, et al. Surveillance for healthcare-associated infections: Hospital-onset adult sepsis events versus current reportable conditions. Clin Infect Dis. 2021; 73 (6):1013–9.
19. Mexican Social Security Institute. Health Information [Internet]. Mexico: IMSS; 2022, [Accessed December 29, 2022]. Available from: http://infosalud.imss.gob.mx/
Citation
Medina-González A and Ruíz-Valdez CA, Impact of healthcare-associated infections on hospital costs, length of stay, and mortality, ERSJ 2026,1(4) 162-174
Academic Editor: David Alejandro Cabrera Gaytan, Received: 2026-march-02 Revised: 2026-april-07 Accepted: 2026-april-14 Published: 2026-april-18